The Denmark study used super sensitive tests.. MPNs may be far more common than current info suggets.
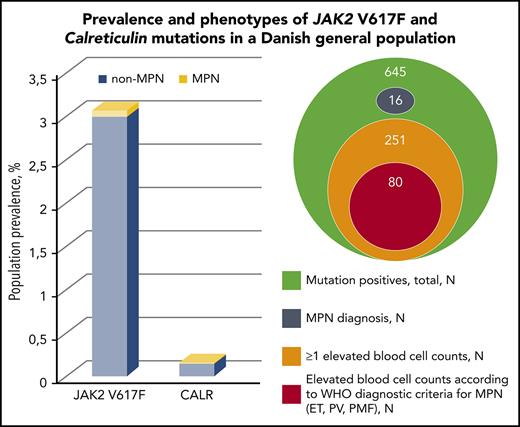
The image here shows 3% have a Jak2 mutation even as most of these have no MPN Dx.
Their cutoff of 1% (orange circle) still includes way more than MPN with Dx (grey circle)
Highlights:
Their point is all these are at risk of high bloods and MPN.
The authors suggest even very low alleles may retain risk.
They also say CALR is more likely to turn into MPN.
--
ashpublications.org/blood/a...
Survey of 19,958 adults:
<<In a population-based screening of 19 958 adult citizens by highly sensitive ddPCR, we found a novel CALR population prevalence of 0.16% with mean allele burden of 7.5% and a JAK2 V617F population prevalence of 3.1% with a mean allele burden of 2.1%.>>
So Jak2 mutations are in ~3% of everybody. Bad habits added to the risk of having a mutation.
CALR is more likely to turn into MPN:
<<suggests that a higher percentage of the CALR positives in the general population evolves into MPN compared with JAK2 V617F positives>>
With any Jak2 mutations risk to become MPN is high:
<<high hazard ratios of 11 and 12.9 for hematological malignancies in individuals with detectable mutation found in the above-mentioned CHIP studies>>I think CHIP is a sort of pre-or-undetermined MPN. But I think these studies were not as sensitive as the present one so may have not caught the very lowest alleles.
This study found much higher prevalence of Jak2 in the population likely because its high sensitive test:
<<The JAK2 V617F prevalence of 3.1% in our general population study is 3 to 30 times higher than in earlier reports>>
MPN may be much more prevalent than thought:
<<If just half of the 80 high-risk individuals with elevated blood cell counts meeting diagnostic criteria turn out to be true MPN patients, the MPN prevalence in our study population increases 350%.>>
--
MPNs have low cholesterol:
<<The lipid profile with low cholesterol values in almost all mutation-positive subgroups is in accordance with observations from MPN patients>>
This is news to me. I do fit this profile.
Any driver mutation may increase odds of MPN:
<We therefore suggest that individuals with a driver mutation, even at a very low mutant allele burden, are considered MPN-risk patients.>>
Maybe any therapy needs to get get rid of all of it to be fully curative.
