A few weeks ago I wrote a post describing an app that I'd written to add together the contributions made by the various anti-Parkinson's drugs that we take. It used the idea of levodopa equivalent dose as a common denominator. For instance, 1mg of rasagiline makes about the same total contribution as 100mg levodopa (taken with carbidopa). This approach can be improved by taking into account the timing of the doses and the different durations of effectiveness of the different drugs. For instance, rasagiline is effective for the whole 24 hours, whereas levodopa lasts for about 4 hours. Roughly speaking, therefore, levodopa is 6 times stronger than rasagiline, but the rasagiline lasts about 6 times as long.
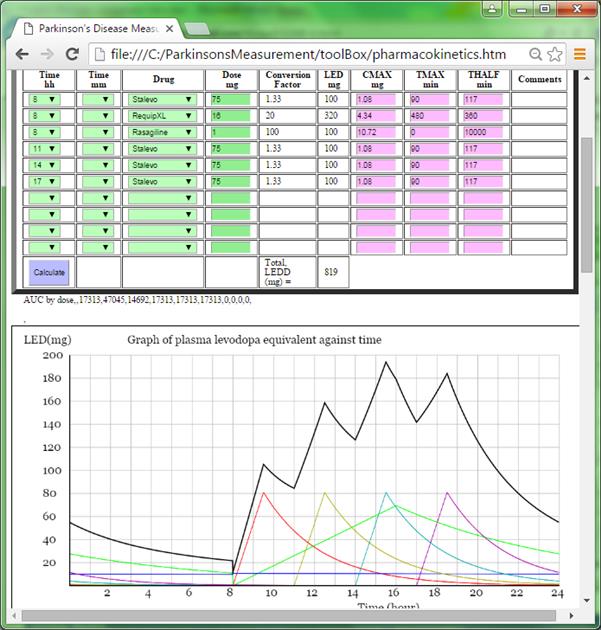
I've written an app to do the calculations and draw the graphs. You just enter the times of your doses and what they contain. See:
Unfortunately, there's no agreement in the scientific literature as to the exact pharmacokinetic parameters to use. I've chosen default values that I think are reasonable, but you can override them if you wish.
John
Written by
johntPM
To view profiles and participate in discussions please or .
John, obvious that you have put together a marvelous analysis. I would suggest a perspective on the label you use on your graph....""Equivalent Plasma Levels" As I follow your description of your analysis your measurement. seems to be drugs scheduled to be taken is your measure? (an interesting measure in itself).
My perspective, is a discussion with my Neurologist when planning my meds.
He indicated that an important issue was passage of the meds from the stomach or small intestine into the body, and then movement of the meds through the blood brain barrier. He indicated that this varied both within and between individual Patients.
Y our graph is labeled "equivalent Plasma levels. Does your analysis account for the variability discussed by my Neurologist?: And are you suggesting an effect within the Brain Blood Barrier?
Regarding your consultant's comments about variability between people and differences over time for one person. He is, of course, right. The model comes with default pharmacokinetic (what the body does to the drug) parameters. I was surprised at the size of the variation of these parameters both within and between clinical trials. In order to cope with this I built in the facility to override the defaults - just type in the values you want changed in the purple boxes.
The only effect within the BBB that I've considered is the role of rasagiline as a MAO-B inhibitor. By reducing the amount of dopamine that would otherwise be destroyed, rasagiline has a similar effect as would come from a dose of levodopa. Strictly speaking this is a pharmacodynamic (what the drug does to the body) effect. Pharmacodynamic effects are otherwise not addressed by the model.
Where I think the model is weakest is that it does not include any endogenous (local) dopamine generation or dopamine reservoirs in the remaining functioning neurons.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.