This post is in response to a couple of recent posts highlighting concerning changes in the effectiveness of our monoclonal antibody armament against new COVID-19 variants:-
A COVID treatment wanes: New variants outsmart most monoclonal antibodies : NPR
healthunlocked.com/cllsuppo... by patagozon
4 of 5 treatments for covid in immunocompromised being removed in NHS
healthunlocked.com/cllsuppo... by Harvist
sparkler and cujoe have also noted the changes in the effectiveness of COVID-19 medications and CLLerinOz summarised them in a reply to our pinned post in SARS-CoV-2/COVID-19 information in the last week here: healthunlocked.com/cllsuppo... healthunlocked.com/cllsuppo...
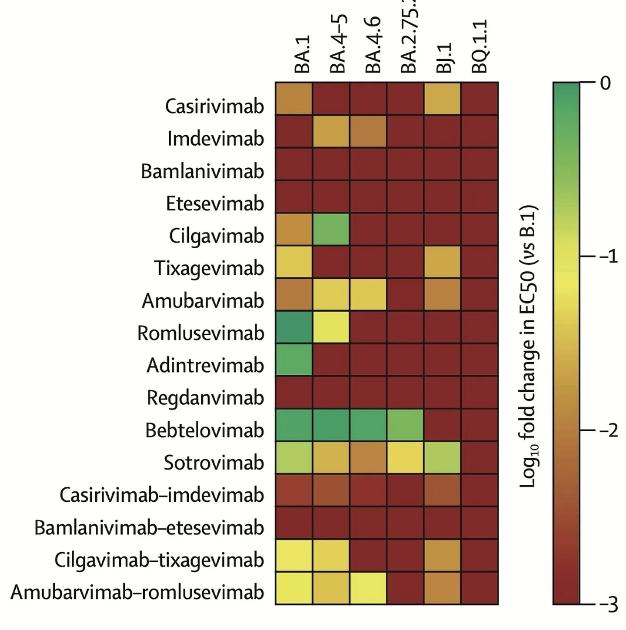
Dr Eric Topol illustrates the worrying situation in his Substack article The BQ.1.1 variant story erictopol.substack.com/p/th... with the accompanying graphic, where he says, "A new report by Arora and colleagues from Germany compared resistance to monoclonal antibodies for many of the most troublesome new variants (mutation map of spike protein below) and, unlike the others assayed, showed that BQ.1.1 demonstrates resistance to all available monoclonal antibodies."
Later in his article, Dr Topol notes "Under pressure from prior infections, vaccinations, boosters and combinations of these, the virus is having a harder time finding new hosts. To date, BQ.1.1 has not been able to induce a new wave in 2 countries, a very positive sign. Sure, there are Omicron lineages with 7 mutations on top of BA.2, like CH.1.1 and BQ.1.1.10, and 8 or 9 mutations (XBB.3 and 4) but are they going to look any different? You might think that BQ.1.1 would qualify as an acid test and so far its outcome looks far more favorable than initially projected. For further context, all of this is happening with minimal mitigation, such as the very low use of masks or avoidance of indoor gatherings. No less in colder weather, heading into winter." (Though as I have recently posted, it's high or low indoor relative humidity that increases the spread of the coronavirus that causes COVID-19, more so than the season. healthunlocked.com/cllsuppo....
Dr Topol does share some good news with regard to the bivalent booster.
There have been 2 reports that the BA.5 bivalent booster has some neutralizing antibody cross-protection against BQ.1.1. First was Emory’s report, that showed a >5-fold increased neutralizing antibody response with the bivalent vs BQ.1.1 as compared with a single original booster.and then the U Texas Galveston Shi lab report with about a 5-fold increased neutralizing antibody response for the bivalent to BQ.1.1 compared to the monovalent, original booster. Both of these studies showed a similar bivalent benefit vs. BA.2.75.2, a variant in the wings that could pick up steam in the months ahead.
He also specifically addresses the concern of our community.
Another concern is that BQ.1.1 is going to cause some trouble. It has blown through Evusheld protection, a vital help for immunocompromised people, and left us without a monoclonal antibody treatment that works for people at high-risk not responding to (or unable to take) Paxlovid. Sadly. we see no new monoclonal on the short term horizon to take their place, even though so many very broad neutralizing antibodies (with potential of being variant-proof) have been identified in many academic labs.
Remember, the size of the SARS-CoV-2 virus hasn't changed. Well fitted high filtration masks (N95, FFP2, etc) work equally well across all variants ") . As Dr Topol closes, And, of course, there are things you can do to maximize protection (like a bivalent booster and high quality masks).
. As Dr Topol closes, And, of course, there are things you can do to maximize protection (like a bivalent booster and high quality masks).
Neil
