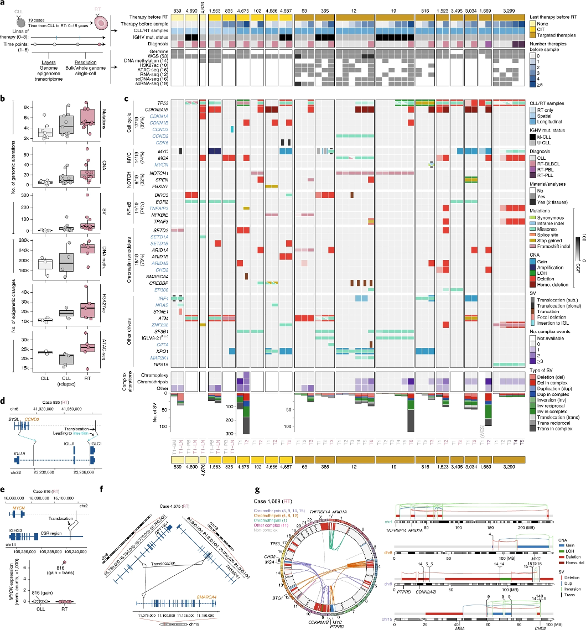
Very interesting article on TR with Dr. Elias Campo among other doctors. Article published by the journal Nature. Posted on August 11. Read it because it gives a lot of information and within this study we are myself and two other people from this group among other cases that we offered ourselves for study. Many of you will see yourselves reflected in this article.
nature.com/articles/s41591-...
Richter’s Transformation Facebook
