"We aimed at developing an IPS‐A for time‐to‐first‐treatment (TTFT) prognostication in stage A CLL patients.
Conclusions: Among stage A CLL initially managed with active surveillance, the IPS‐A allows to inform upfront patients, physicians and researchers about the likelihood of disease progression."
My absolute lymph count is 3.01 and my lymphocytes relative is 34.40 % all my CBC are in normal range. But my hemoglobin is slightly elevated and I’m not sure why but it’s just above normal and has been for on the last 6 months. Prior to that that was always in normal range.
Correct in most cases sll shows normal blood cbc. The B cell is in the lymph nodes. It can turn into CLL if the absolute Lymph is over 5( 5,000 ) they also look at platelets closely along with neutrophil count.
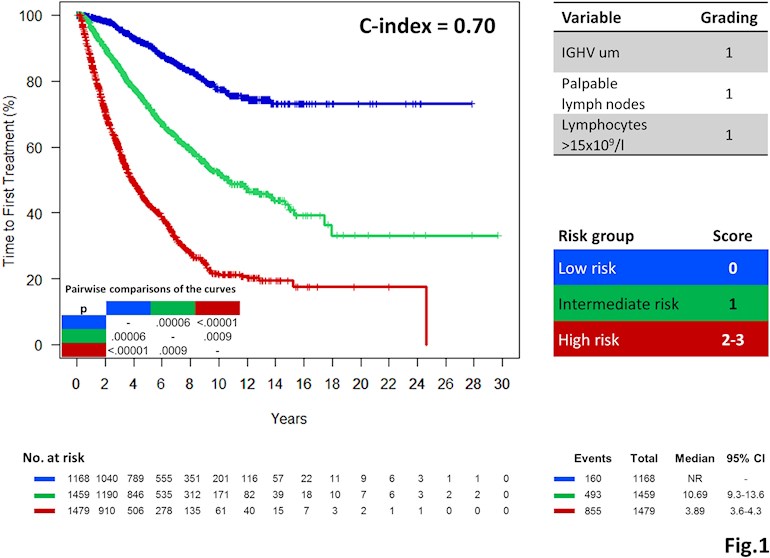
Slightly worried to see that in Binet A lymphocytes over 15x10**9/l seem to put me Intermediate Risk group as I had understood that “they” only really got interested at 30. Any comments?
I think "they" pay more attention to lymphocyte doubling time after ALC reaches 30, because it can be sign of the disease progressing (possibly requiring treatment).
In this case, this group was trying to classify patients by time-to-first-treatment so 15 was the significant level.
"Among intermediate‐risk patients, median TTFT was 10.69 years "
Also it appears that ~1/3 of intermediate-risk patients have never required treatment.
I've never liked this sort of graph and statistical analysis. Our first instinct is to try to find ourselves on the graph. We often fail.
I also don't like this particular paper because of dense, poorly worded statistical jargon, such as:
"Backward elimination was used to derive the final model, and variables resulting non‐significant in more than half of the validation cohorts were excluded from the model."
That surely means something to a statistician, but I'll wager that the average clinician and patient find it baffling, even if they once had classes in statistics. We just nod our heads, and assume the authors know what they are doing. A few out there probably DO know what the authors are doing, and I hope they will weigh in.
I fear that such analyses ignore many other factors which could change prognosis for an individual for the better or worse. i.e. It's only true for the few factors that it analyzes. In defining the forest, it loses the trees.
It provides no actual information for specific individuals.
It's contrary to the growing trend toward precision medicine. It will leave clinicians stumbling to explain why a particular patient varied from some predicted value - and will make those clinicians look worse than they actually are. Don't get your hopes up for any better numbers anytime soon, though. It's too complicated still, I think. Give more weight to good news, and less to seemingly bad.
I will note that the c-index is a key number here. An ideal c-index is 1.0 - never achieved in any such analysis. Random chance would have a c-index of 0.5. Values smack in the middle between 0.5 and 1.0, as in this paper, are fuzzy. It would have been nice to see numbers above 0.8. I think that limiting the results to 3 groups made things fuzzier.
Also look at the 95% Cl (confidence interval ) values. They have a range of years, but the low risk group didn't reach it:
"By compiling the training and validation series to narrow the confidence interval of the estimates, among low risk patients median TTFT was not reached and at 10 years 77% of patients were treatment free. Among intermediate‐risk patients, median TTFT was 10.69 years (95% CI 9.31‐13.60). Among high‐risk patients, median TTFT was 3.89 years (95% CI 3.56‐4.30) (Fig. 1)."
Turning the low risk group around, 23% DID indeed enter treatment by 10 years. That's a pretty big number, I think!
The obvious problem here is that recent studies necessarily won't have that long term info. We're seeing more patients diagnosed at earlier ages. They may not have as many co-morbidities as older patients, and clinicians may be more likely to delay treatment. Conversely, over the period of the studies cited, criteria for treatment may have changed.
Treatment is also not the same as overall survival. But I'm glad they used TTFT.
It makes me want to take some classes in statistics.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.