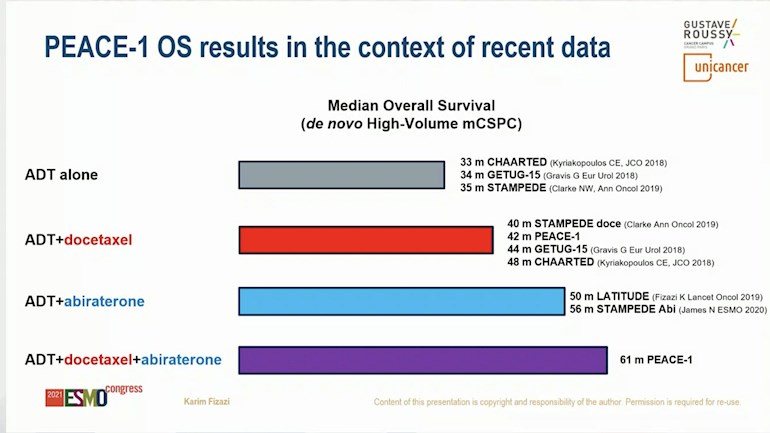
I promised I'd update this as more info came in. The lead investigator, Karim Fizazi, presented a chart comparing the overall survival in men originally diagnosed with high volume (≥4) distant metastases and treated with both medicines. Their overall survival increased more than with either alone.
PEACE1 - the advantage of combining d... - Advanced Prostate...
PEACE1 - the advantage of combining docetaxel and abiraterone in men newly diagnosed with high volume metastatic PCA (update)
Written by

Tall_Allen
To view profiles and participate in discussions please or .
Read more about...
88 Replies
•
I wonder if taking the docetaxile followed by zytiga is considered in the same group? Husband had heavy load of metastasis and was started right on chemo then zytiga was started. We tried to get both at once but standard of care prevented it. Most metastasis are gone now. Four years ago diagnosis.
in reply to Cynthgob
I'm wondering the same thing since I'm also in the group that did early Docetaxel followed by Zytiga.
I've had an excellent response so far and wondering whether those who had early Docetaxel followed by Zytiga will have similar outcomes to those who do them both upfront. Guessing they probably won't ever be compared.
Cynthgob in reply to
Looks like the same time diagnosed. And very similar treatment. Had to go off Zytiga and dex. Now starting clinical trial with Lu-177.
in reply to Cynthgob
I've definitely gotten more out of Zytiga than most so starting to wonder when it's going to come to an end. Hopefully I'll be lucky and keep going on Zytiga, but probably will do LU-177 next if it's FDA approved by then.
in reply to
I think there's a guy going on 8+ years od ADT + zytiga. Hopefully you're in that group. Lulu700 is similar but his second generation adt is no longer marketed but he's been going 6+ year's.
in reply to
Thanks, hope I keep going. I'm really careful not to brag about my results like some of the alternatives crowd do.
Just for everyone's information: I have a reasonably healthy diet, but eat meat, dairy, drink alcohol at times, only take a single multivitamin each day. No special diet or supplement protocols, just a good response from proven treatments. And so far, I'm damn lucky!
in reply to
I understand where you're coming from. I take a few supplements but generally try to exercise and eat well.
Not vegetarian. Lifes too short to not enjoy a Ribeye, lobster, scallops ribs etc. Besides, I just got a echo 2d cardiac dappled and CT cardiac calcium test done. My GP says everything looks real good and I have a consult with the cardiologist in early Nov. After 2 + years of ADT and zytiga I wanted to see if anything was going on cardiac wise.
in reply to
There's a lot of quality of life involved when it comes to eating the foods I like. I see a lot of people giving up foods for some theoretical and unproven advantage.
There's what I call the "diminishing returns curve" that I always keep in mind. At some point you are putting a lot more effort, energy, time, money etc, for smaller and smaller gains. Having a diet that's reasonably healthy is close enough to an extreme diet and you still get to enjoy the foods you love. I can't imagine saying on my death bed "I really wish I had eaten less pork ribs".
MarkBC in reply to
gregg57: I really like what you say and I follow a similar philosophy with regard to diet. Don't be afraid to brag about your results. We all need to hear good news stories. I'm still castrate sensitive after three years with a PSA of 0.1. I'm enjoying every day, including a few gin and tonics, the odd steak, and even some desserts.
CAMPSOUPS in reply to
I may have said this before but with a couple estimated expirations looming over my head now is not the time to set up an apothecary in my home.
I guess fortunate to have always ate relatively healthy but do not sacrifice the pleasure of good food no matter what it might be.
Boywonder56 in reply to
Im going to do same....heart doc said my heartcwasnt going to be the death of me after 2yrs adt..been 4.5 now so will see if same otherwise i take no supplements drink some pot most nites to sleep....
Forgot comma after drrinks some, if you care.lol
I care............Missing commas are a nuisance...........but missing periods are hell..............
Good Luck, Good Health and Good Humor.
j-o-h-n Monday 09/20/2021 7:29 PM DST
in reply to Boywonder56
The cardiac calcium test isn't covered by insurance but it only cost roughly $100 (mine was $108). It reveals how much calcium is deposited in the the arteries around the heart.
The 2D Echo Cardiac Doppler test can reveal any issues with Heart and Arteries.
Apparently there is history of congenital heart disease in the family.
5 years ago a younger brother died of a Aortic Dissection and my older sister just had heart surgery to fix an issue with her aorta.
My GP wanted to put me on a statin at my last visit but I pushed back and he wrote the scripts for the 2 diagnostic tests. End result. It seems im in really good shape heart wise and don't need a statin.
I'm 2 for 2 now. First was a agent to battle bmd issues from ADT. I said I wanted a dexa scan first. Good bmd after a year on ADT so no meds needed. Now the statin. I like my GP alot but alot of Dr's he follows the guidelines but is open to wait for tests to confirm.
BTW. Little know fact. Statins don't work by lowering cholesterol. All of the benefits come from the anti-inflammatory action. And Total cholesterol is being pushed aside by the cardiac calcium score which the CT Cardiac Calcium scan provides. Basically, why take a statin if the arteries are clear.
Long winded but some additional details can help.
Try melatonin for sleeping. I take 6mg at night and I sleep real well at night now. A good anti inflammatory too.
Cynthgob & Gregg57-
When PEACE1 began, standard of care (SOC) was ADT only. Later SOC became ADT+docetaxel (doc). When that occurred, the overall survival test for abiraterone (abi) effectiveness became abi+doc+adt vs doc+adt, which now turns out to be 61 mos vs 41 mos, respectively. I know this doesn't really address your question.
When doc is used in the absence of abi, some cancer cells "protect" themselves by undergoing a transition called "cellular senescence." (This also occurs with abi in the absence of doc). Senescent cells do not rapidly divide but they do metabolize nutrients. They also influence other cells to become cancerous. Because they don't divide, they are invulnerable to chemo like doc and to medicines that influence how androgen receptors act, like abi. (BTW- during this phase they do not grow blood vessels so they release little or no PSA, so those patients who become complacent by low PSA are misguided.) Eventually they come out of hiding and start to divide again, making them vulnerable. Rising PSA is the signal that those cells may be vulnerable. So you have to wait for that signal.
There is a clinical trial of a cocktail with anti-metabolite types of chemo that may target senescent cells.
clinicaltrials.gov/ct2/show...
Would you be able to share any insight as to the possible efficacy of adding do eta all to abi now after being on Lupron and abi one year. (, one pelvic bone met showed originally on conventional imaging. Psa was 15 before treatment). Also had SBRT of prostate and the met. Psa now undectable. No pain. So far we were told Peace study is inapplicable and don’t add the chemo yet.
Whoops, I think you answer this question below.
in reply to Tall_Allen
There is much literature on the benefits of fasting. One such fasting regiment is the 72 hour fast. Apparently, one of the benefits is the body uses senescent cells for fuel after 48 hours. My understanding is this is part of the anti-aging effect of fasting.
My issue is I can't seem to find any information on what senescent cells are broken down during the fasting period. My feeling is cancer senescent cells would evade this cleansing process.
Do you have any thoughts on this?
j-o-h-n in reply to
Yes I do, but I'm keeping them to myself........... p.s. I normally fast between meals...........
Good Luck, Good Health and Good Humor.
j-o-h-n Monday 09/20/2021 7:45 PM DST
in reply to j-o-h-n
I thought you un fastened your belt between meals.
j-o-h-n in reply to
A belt implies that I wear pants.... You don't think I wear a belt while I'm naked, do you?
Good Luck, Good Health and Good Humor.
j-o-h-n Monday 09/20/2021 10:00 PM DST
Purple-Bike in reply to
TomTom1111, indeed this is the huge question. Autophagy progresses to apoptosis after about 3 days of fasting, clearing out senescent cells - but does this clear out cancer senescent cells? After a quick search I too couldn´t find anything on what types of senescent cells are broken down, but let´s continue! Perhaps a contact with one of the researchers e.g. dr Longo might reveal something, although discouragingly he didn´t delve on the issue in his recent major article in Nature Aging 1.
I´m doing a 19-hour daily fast and if a search shows a possibility of cancer senescent cell removal in a 3-5 day fast I will take up the challenge. Perhaps anyway, if strong additional health benefits of multi-day fasting compared to IF show up in the search. Thank for posting, it inspired me to take up this tack.
in reply to Purple-Bike
Thanks for the reply. I do the 16:8 IF right now...started doing it roughly 2 years ago.
I think it helps. The longer fasting I'm waiting until October when my last 3 mo Eligard wears off. But in the mean time I'm going to start doing 24 hour fasting first to get the body in shape...then a 48 hour and then I'm thinking of incorporating monthly 72 hour fasts starting in the new year. My personal opinion is that the natural therapies will only work in very low burden cancer patients. So if the treatments can get a patient to that state, these other treatment modalities may have a positive outcome....only time will tell.
Purple-Bike in reply to
Hunger, for me at least, will be the big challenge for multi-day fasts. I´m ravenous after 20 or so hours. I imagine getting to sleep will require high-dose sleeping pills. In the mean time I will be reading up on the benefits of 72+ hours of fasting.
TA, this is what I also learned from Dr Carlos Alemany in Orlando. I mentioned the PEACE Trial and he said because I started w ADT + Abi, to give Docetaxel would not accomplish anything as cells are in senescence. He said once PSA begins to rise, only then would Docetaxel give a good response. I guess Dx in October 2020 was a little early for PEACE Trial data? Wish I had started with Docetaxel, then Abi & ADT. The order of which first is key, not just getting all 3. Mike
St Pete
My "bias" is to start with docetaxel when one is at one's peak physically. It makes little sense to me to wait until there is significant progression after therapy to start docetaxel.
dhccpa in reply to
Were you ever on Lupron alone for a period of time early on?
in reply to dhccpa
Just the first month. My oncologist was pushing me to do Docetaxel chemo with ADT, but I initially refused. Early Abi was not yet approved. After a month on ADT, I decided to do the chemo.
dhccpa in reply to
I have been on Lupron alone for three years now. Docs were divided on doubling up back then so I've stuck with it. PSA is 0.6 as of last week but I may proactively do 6 rounds of docetaxel if I feel inspired.
DarkEnergy in reply to
Absolutely, Schwah and myself, have been favorable to combinational therapies based on our experiences and research, For me, Lupron, Zytiga and Docetaxel concurrently has me on vacation for a year, with holding undetectable PSA at "the moment". Our Prostate Cancer is unique to all of us, so it's just my experience of one.
Thanks for posting!
Thanks for posting this!
Same here thanks for posting TA.
For those reading the thread I had Taxotere at DX without Zytiga 😑
I was fully metastatic and high PSA at DX.
Lupron/Eligard and Taxotere.
11 to 13 months after my 6th Taxotere infusion PSA rose from the 8 to 9 it had hovered at after chemo and shot up to 40 between the 11th and 13th month after my last Taxotere infusion. ( I actually felt it in my bone metastases but dismissed it as ADT side effects ).
Began Zytiga 14 months after last chemo.
Cant turn back the clock. Hope I get a lot of time/mileage out of Zytiga.
Began Zytiga this past early August. PSA 9 days into it fell from 40 to 16.Met pains diminished greatly after 3 or so weeks. Back to rubber legs or legs that just came out of the sauna. Not painful however have a "hitch" in femur hip joint..have to be careful.
Next PSA will be next week.
I remember my first 6 weeks into ADT + ABI etc…I felt like tottering tower from the weakness in my pelvis. It was a curious but hopeful time as I slowly regained my strength. I remain steady on my feet now but not as comfortable hiking over rough ground…I’ll take that over what we all understand as the advancing alternative. PC has been a blessing in some ways reminding me how precious remission from its ravages reawakened life’s simple appreciations.
I fight on taking time remembering others not so lucky trying my best to live up to blessings of struggles I’ve not had to face.
Thank you 🙏
Hi TA. Thanks for posting. Does "cellular senescence” also occur with ADT + Xtandi? I have been on ADT + Xtandi for 18 months. My PSA has been < 0.10 for 12 months. Should I talk to my MO about Doc at this point? I have an appointment this week. Thanks
Yes - all the second-line hormonals cause it. It would probably be pointless to start on doc until cells are replicating.
As the evidence continues to mount showing early combined use of PC drugs leads to better outcomes, we continue to have numerous participants on this site, promote the sequential use of these drugs in the misguided effort to “save” drugs for future use. I am certain that this is a good faith belief, but I hope this newest information will finally put an end to that thinking. By the way my Dr (Mark Scholz) advised me to use all three at the first sign of my own metastasis over 4 years ago, long before any of this evidence was in (look at my old posts explaining his thinking). My second opinion at UCLA was 100% against this approach since no compelling evidence was in at the time to support such a protocol.
Schwah
It is not just forum members. Many well-respected MOs (including mine) apparently continue to favor "saving" drugs, for use after the failure of ADT.
What evidence does your MO base his position on and how does he reconcile that position with the numerous studies which clearly show the opposite is true?
Schwah
I've run into the "save it for later" argument a few times. It is easily dismissed because it is (1) always true that the same drugs used earlier have more benefit and fewer side effects than if used later and (2) the pace at which new more effective drugs are introduced tells us that there will be more options later. Any reasonable MO will agree. I've never had it be an issue.
I have yet to discuss it with him, but I would bet it is along the lines of what Tango65 is saying below, including the part where "patients will not be subjected to the undesirable side effects of chemo and abiraterone at the same time."
His PA has suggested that is merely his default position, and that he will have no problem doing the described combo if a patient wants it. I should add, my own met volume was not "high" at diagnosis (but my recently spiking ALP during a failed tE2 attempt at ADT did indicate is was increasing).
Personally, I intend to add abi to my firmagon ADT after several months, then add doc after several months, just so that I can (hopefully) distinguish which treatment regimes might be the cause of any severe side effects (should they occur).
Sequencing does not work the same way for the reason I described in my reply to Gregg57 and Cynthgob above.
All side effects are worse later.
There is a danger in drawing sweeping conclusions without clinical data. It is not always the case that combos work better. I want to just throw in 3 examples where a combo did not work:
(1) docetaxel+enzalutamide (ENZAMET)
(2) docetaxel+apalutamide (TITAN)
(2) abiraterone+enzalutamide
While Dr. Scholz luckily happened to be right about doc+abi, he would have been wrong with doc+enza/apa or in combining abi+enza. He was wrong about combining a 5ari with ADT. There's nothing wrong with predicting wrongly, as long as clinical evidence corrects the wrong assumptions. That's just good scientific practice.
You are correct that there are risks to combining drugs without clinical proof. I was aware of those risks and willing to take them. I was a long time real estate developer and I also like to gamble a bit. So I think I am pretty good at sizing up the risks with the data available and making a decision for myself. I of course hope that my decisions will increase my life span but I am prepared to live (or die) with any negative consequences of my decisions. You have been there a number of times to help me size up my risks and for that I am grateful.
Schwah
I used to be an honest physicist.. then many years in sort-of honest oil & gas... but the I became a property developer... now I’m pretty sure PCa is the universe’s way of dealing with developers!
Ouch….hope not.
Hi Schwah,
Remember when we posted taking ADT (Lupron), Zytiga and Docetaxel concurrently, folks thought we were nuts... ")
Yup….who was your MO that recommended that protocol.
Schwah.
Actually, I suggested it, the MO, Dana-Farber's Dr. Mark Pomerantz, said absolutely and ordered it.
This is not a comparison among different arms of the same randomized control trial. This is a comparison among historical data from different studies.
Nobody knows if doing abiraterone and then docetaxel or doing docetaxel and then abiraterone have or not the same results than abiraterone plus docetaxel and most probable less side effects.
If you look closely at the second bar above, it is a randomized arm of PEACE1: OS of 42 months for doc vs. 61 months for abi+doc. So patients lived over 1 ½ yrs longer if they used the combination. Doc and abi only add 3-4 months to survival when used for mCRPC, so this is a huge difference.
Side effects are much less and comparable in degree (but different in kind) to abi side effects when used upfront.
Right, but the arm ADT + abiraterone followed by docetaxel does not exist.
If you go by historical controls, Stampede showed 56 months for ADT + abiraterone alone (3rd bar) in your post only 5 months difference with the PEACE trial. The problem is that we can not compare 2 different studies, so we do not know.
Until we have a RCT comparing adt+ abiraterone followed by docetaxel vs adt+ abiraterone+ docetaxel, we can not advocate to change the SOC to a more toxic combination of drugs.
ADT + abiraterone followed by docetaxel may be as effective or more effective than adt+ abiraterone+ docetaxel and patients will not be subjected to the undesirable side effects of chemo and abiraterone at the same time.
But we do have ADT+doc. And we have another study that directly randomized patients to ADT+doc or ADT+abiraterone and the OS was equivalent:
Yes Tango 65. I fall into this unstudied group. I was started on Lupron + Xtandi (then Zytiga/Abi) in 1st month. No Docetaxel. Now I am told Docetaxel will have to wait as cells are in sennescence with PSA down to .67. I am all for (although not anxious) Docetaxel, but now we know since ASCO this year that Docetaxel upfront is superior. Sorry they didn’t include our case in study with all 3 but in different order. I was only Dx last October 11 mos ago but PEACE Trial released this year.
Mike
St Pete
TA,I never understood this overall survival thing. I don’t have a grasp of what it actually means. Are we discussing 10 months of ACTUAL time on earth( I know it’s avarge)? or this to just give doctors a way of evaluating which is better?
When I hear this drug gives a 3 months better survival, is it worth it?
It is median survival - half live longer, half die sooner. For the ones who live longer, just how long they live is an open question - they usually stop the trial at that point.
So, in this case, half the men who started with doc+abi lived 5.1 years or more. When these drugs are given to men who have progressed to castration resistance, the increase in median survival is about 3-4 months vs an increase of about 2.5 years if used upfront.
Great post.. Just curious. I had docs Nov-Mar, brought psa down from 1000 to 9, held there for 2 Mos, also on eligard. Psa went to 36, with new bone Mets in hips/ribs. Put on abi, psa back to 7. Does it do any good to ask to add doc while doing this? How about if psa goes up, keeping on abi and adding doc any good? Mostly interested in first question
It's a different situation, and I really have no data on combining them for mCRPC. But it is worth a conversation.
Hi RunThru. I had ADT and Doc in 2015 following the CHAARTED data. Oncologist then allowed me to have 9 more for a total of 15 Taxotere sessions. PSA went from 840.2 to 0.7 with a nadir in the Summer of 2017 at 0.1 Had another 6 doc that ended in 04/2021 and PSA got to the lowest in 3 years at 2.2. And an Axumin scan showed lower activity in the 2 iliac lymph nodes.However, PSA jumped from 2.6 to 3.6 in a month and will have another Axumin done. Just had Lupron 3 monther and hope to restart Abi and/or Xtandi - both failed in 20201
Fight on
Randy
Allen,Thanks much for posting that. I think I asked before but for men already diagnosed (back in 2012, 4+3=7 in two samples, Mets in 5 places) this study does not apply? I often think misguidedly I am more like a newbie rather than a PC veteran as my PSA has been undetectable for 7 years now, on Zytiga alone. Might ask my Onc anyway about adding Doctaxel..or maybe not. In any case, I get a clearer picture of whats going on with me with your "cellular senescence." explanation, so thanks for that.
You are correct that it does not apply to you now.
Is erleada not as good with >4 mets?..i know the titan included both high and low volume cancers...i was <4 metz and have done well slow moving psadt...i am still in open lable faze....
Hi Tall_Allen, I am in the group under Stampede/Chaarted. (Treated 2017-2018) Recently my PSA spiked due to ADT holiday. Back on ADT and PSA has come back down again. I am still castrate sensitive and the Onocologist would like to add Apalutamide. Would Abiraterone be a better choice if my next scans show any activity with my distant metastases.Thanks,
For some unknown reason abi->enza lasts longer than enza->abi. The same may be true if apa is used instead of enza, but I haven't seen any evidence of that.
Great post/article, TA. I think that this study nicely relates to earlier STAMPEDE and LATITUDE study findings.
BTW, PEACE1 screened for new patients with "excellent performance status"... for those of us not completely familiar with the "performance status" term, here is an excellent summary from the Journal of the American Medical Association (JAMA):
jamanetwork.com/journals/ja...
"Excellent performance status" means a "0" on the Zubrod Scale. Theoretically, the men in the PEACE1 study had higher baseline health "reserves" to take on the significant physiologic impact of treatment. Honestly, I'd like to have seen a more realistic study cadre made up of Status 1 or 2 participants as was used in both STAMPEDE and LATITUDE. - joe m.
Newly diagnosed patients usually have excellent performance status, and ALL of the PEACE1 patients were de novo. ¾ of STAMPEDE pts had excellent performance status. In LATITUDE about half the men with worse performance status, and 80% were high volume.
Thank you T_A. Clarifying the role of PC senescent cells is very valuable consideration. I am wondering what non-de novo situations with PSA taking off sharply after a time of indolence, and or new crop of mets on scans, would indicate emergence from senescence. And would that suggest that could be a good time for aggressive chemo+abi+ADT for similar reasons?One such that comes to mind is those men who do badly on BAT with rapid progressive rise in PSA? Or the end of a long IADT “holiday” with PSA rising from restored testosterone?
I agree that the combo is something to consider when the cancer "wakes up." BAT may help change cells to a non-senescent state - i don't know - if so, they may be more vulnerable.
Loved this part... 😲 "The authors found that patients born on a Monday benefited the most from abiraterone, and it was statistically significant, while patients born on a Friday had the least benefit, and it wasn't statistically significant."
Yes! It is a warning about subgroup analyses, especially if unplanned. Subgroups are often underpowered to draw conclusions from. As it turns out, abi IS effective in the M0 population.
I haven't looked the other trial numbers for ADT + Docetaxel, but the CHAARTED trial (I believe one of these oldest) had this update:
At a median follow-up of 53.7 months, overall survival (OS) remained significantly longer for the 397 participants who were randomly assigned to receive ADT plus docetaxel 75 mg/m2 every 3 weeks for up to six cycles than for their 393 counterparts given ADT alone, at a median of 57.6 versus 47.2 months, and an HR of 0.72.
This was also the case for the subgroup of patients with high-volume disease, defined by the presence of visceral metastases and/or four or more bone lesions, of which at least one had to be located outside of the vertebral column or pelvis. Specifically, OS was a median of 51.2 months for the ADT plus docetaxel group and 34.4 months for the ADT alone group, giving a significant HR of 0.63.
oncology.medicinematters.co...
Also:
onclive.com/view/update-sus...
I realize it's only one of the trials, but if this is correct, a median OS of 51.2 months for ADT plus Docetaxel would be slightly better than ADT+ABI in LATITUDE (50), but less than STAMPEDE (56).
Tall_Allen in reply to
I would call those the same. A randomized comparison was done within STAMPEDE that found they were the same.
ncbi.nlm.nih.gov/pmc/articl...
in reply to Tall_Allen
Just after I started chemo, early Abiraterone for HSPCa was approved so I didn't have the option to do it instead of chemo. But glad I did and hopefully I'm getting the benefit that's been seen in the clinical trials. Looking likely I'll make 5 years since diagnosis with stage 4.
Tall_Allen in reply to
I always use you as a positive example. NICE/NHS in England won't pay for abi, only doc. In France, doc first seems to be prevalent. In the US, doc first is only used for high volume mets, a mistaken interpretation of the research, IMO. After PEACE1, I think SOC will change around the world.
CAMPSOUPS in reply to
It appears from your bio you started Abi approx. 11 months after Dox ?For me it was about 14 months after Dox.
Seems too that your PSA had begun to rise thus started Abi.
Hope I get a good run on Abi as well. You were among some of the first brothers here I noted with good Tx success when I began snooping around here on HU.
Your Leary Biscuit reply in a thread stuck with me as well. lol.
in reply to CAMPSOUPS
Seemed like I became castrate resistant fairly quickly, then my PSA was doubling every 3 weeks and I kind of freaked out a bit. I was thinking things weren't looking too good. I was really wondering whether the chemo had done anything.
My doctor said he often sees fast rising PSA with patients that do Docetaxel upfront. As soon as I started Zytiga, my PSA dropped almost overnight, soon becoming undetectable. When my doctor saw that he said he expected at least 2 years for me and it's been over 3 now. So maybe there's a more long-term benefit from the early Docetaxel, possibly killing off some of the cancer that are not hormone sensitive.
I remember going to prostate cancer conference and they showed two graphs: one was what they called "overstated benefit" showed the two lines SOC and SOC+ diverting significantly after a short time, but then coming almost together not too much after. Then they had another they labeled "understated benefit" where the two lines divergered slowly but kept diverging quite a bit further out than the first pair. I found that very interesting. I think that early Docetaxel chemotherapy may be in the second group.
Thank you for posting this. I'm new to this sight. It appears that this study doesn't apply to me correct (please view my profile).
No. It only applies to those who are newly diagnosed with metastases. You are recurrent with metastases.
Great review Allen!!
Not what you're looking for?
You may also like...
PEACE1 - the advantage of combining docetaxel and abiraterone in men newly diagnosed with metastatic PCA
about it, as promised. I'll update it as more info comes in....
Abiraterone+docetaxel+ADT for newly diagnosed metastatic men beats docetaxel+ADT (or abiraterone+ADT)
They randomized newly diagnosed metastatic men to either prostate radiation or abiraterone or...
Another victory for \"triplet\"therapy for newly diagnosed metastatic men.
same time, increased survival by over 1 ½ years in men with high volume metastases (we are awaiting...
Abiraterone or Docetaxel: Which Is Optimal for Hormone-Sensitive High-Risk Prostate Cancer?
anyone know if there is proven survival benefit to starting with either one?
Kevin
Newly diagnosed for high grade Prostate Cancer
case\\".
Doctors will seldom do anything more than treating you.
The more you know the better and...