Hello group and as the year start i wish to all peace and love around you.
After my targeted biopsy at G 4+5 and G 4+3 all on one side, with no peri-neural invasion, no seminal invasion and a 17 PSA at the same level for one year... i have been prescribed a PR + ePLND (extended lymphadenectomy) to occur in February. The oncologist and I have discussed the max PR option but he felt (and me also) that it would be best to conserve "options" for the future. This Dr is experienced, he his a researcher on prostate cancer and oncologist-surgeon. He said ihe can spare nerves on the left side but it would not be prudent on the right side (where the G9 and G7 are).
But he also said you need ePLND. The definition speak itself:
The presence of nodal metastases (LN+) remains an adverse prognostic factor in patients treated for prostate cancer (PCa), and, in intermediate and high-risk patients (pts), current European Association of Urology (EAU) PCa guidelines recommend performing extended pelvic lymph node dissection (ePLND) in case of an estimated risk for LN+ >5%
ePLND is recommended as "best practice" for high risk patient as he said. But after reading many of the posts of fellows here and also most of the recent litterature i arrive at a different conclusion. Supporting articles:
The question is the following: Is ePLND more a staging technique than a therapeutic approach ? All the arguments are found on retrospective studies and limited number of patients. 25 % of chance of having node involvement means also 75 % of chance of not having node involvement. My understanding is that if they found after the RARP:
-Postive margin upon dissection of the prostate or seminal vesicles
-Increasing PSA 3 or 6 months after surgery
Then i will need anyway either hormonal or radiation as adjuvant. Maybe i could let the surgeon remove some nodes (limited lymphadenectomy) but not the extended which lead to much more probability of morbidity.
Is it possible that in a near future... a random study would invalidate all the conclusion of the current retrospective studies and claim that there are not so much difference in survival or incidence of biological recurence between having a PLND or not ?
Written by
Northcaptain
To view profiles and participate in discussions please or .
Prostate and any enlarged lymph nodes---yes. LPND up to you, but I wouldn't, Seen to many people with problems later. Looks lots better for you than what I started with. Good luck and keep us posted.
So much people go out to purchase lottery for 1 out of 13 000 000 chance... why should i take so much chance for having long term morbidity with lymphocel and less node to fight and nourish my body...just because i have 20 %? chance (by the book - not proven) to have micro-metastase to nodes ??? or 80 % or not having. I would purchase lottery with 80 % chance of winning.. not with 20 %
I don't know which options you hope to conserve for the future, but there are good salvage options whether you go with radiation or surgery. More importantly, only 13% of the high-risk men who had brachy boost therapy were free of metastases in 10 years vs 46% of those who started with surgery, even if they had salvage radiation. Your oncologist should not be expected to know about this - it's not what he does. You have to talk to an expert in brachy boost therapy like Peter Hoskin.
You are right that ePLND is more a staging technique than a therapeutic approach. Even if he is able to find 40 lymph nodes, that is only a fraction of the pelvic LNs you have. if any are positive (which is likely), you will have to have salvage radiation anyway, and salvage radiation is more toxic than primary radiation. ePLND misses about a quarter of the LNs later found to be positive. Read the section on PLND:
Thanks Allen for your very informed post. Yes i'm aware of the difference in survival and reccurence free between max RT (Brachy boost + primary rad) and max RP (prostatectomy + lymphadenectomy + radiation/hormonal if lymph positive). It seems whatever path is choosen there is some controversy on the way, this might be why the litterature say "there is not a gold standard approach yet for high risk patient".
In the public healthcare ecosystem that i live within, the access to a surgeon-onco is much easier than a top level radiation onco knowledgeable in brachy boost... so this will be the final deciding factor. Here we have access to free medecine but the counterpart is not much choice in the treatment options-unless someone goes to a trial but there are not much in Canada.
I will probably authorize the surgeon to remove 20 nodes but no more.... an intermediary between standard PLND template and ePLND... I'll take the risk... anyway if PSA rebounce after surgery then as you say anyway salvage radiation and ADT will have to be involved in the treatment.
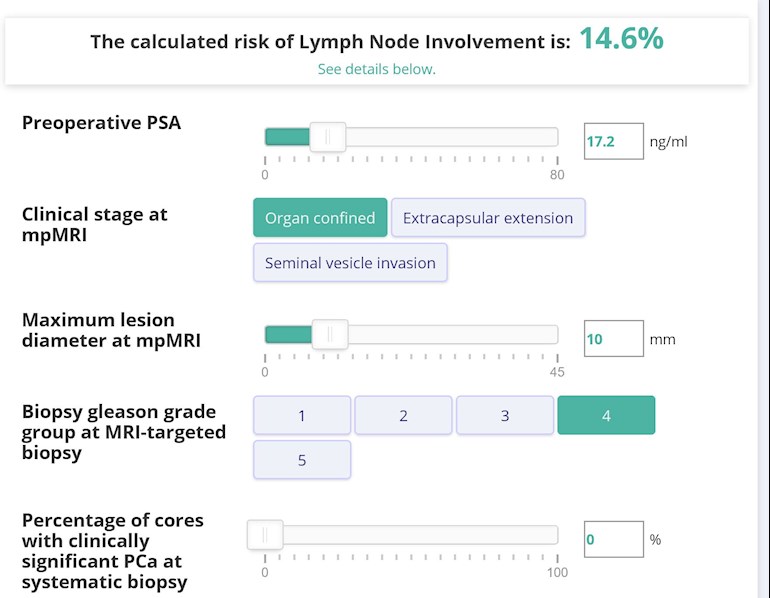
The latest and greatest monogram says 15 % chance for my PSA, stage and MRI. The other one based on biopsy says 25 %. These are probability to have positive nodes....so when you say probably.... you're not following the nomogram odds I prefer to see it as probably i won't have
Sorry - I guessed you were in the UK - my bad. I have talked to patients who were able to get appointments at Sunnybrook and the Vancouver Prostate Centre. At Sunnybrook in Toronto they just completed trials of SBRT for high risk. High risk patients were treated with SBRT only to the prostate, seminal vesicles and pelvic lymph nodes - after 5 years, there were no biochemical failures:
If you're closer to Vancouver, they did the definitive trial of brachy boost therapy vs external beam. I know they have a trial going now utilizing high dose rate brachytherapy in place of seeds.
I use the following nomogram, which seems to have the best predictive power. They consider anything above 7% probability to be high enough to warrant ePLND.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")