Hi all. I'm new to this forum. I'm a 52 year old man. My main health problems have always been unexplained chronic pain and unexplained chronic insomnia, stress, anxiety and depression.
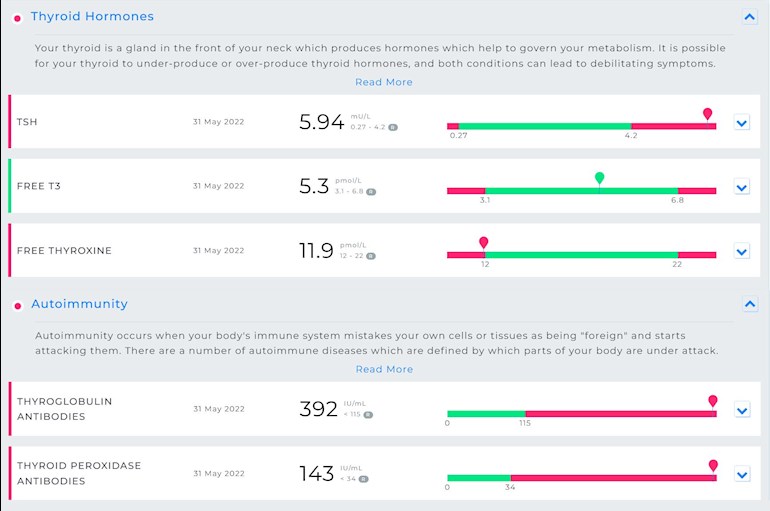
I've had my thyroid checked by Medichecks and they suggest I have Hashimoto’s disease & antibody problems.
I'd value any advice to help me understand what my results mean because I don't know anything about the condition at the moment.
Here are my Medichecks results:
Thank you
Written by
Mr_PSB
To view profiles and participate in discussions please or .
Do I take it that you don't have a diagnosis of hypothyroidism from your GP and are not on any thyroid medication?
These Medichecks results confirm autoimmune thyroid disease, known to patients as Hashimoto's. This is where the immune system attacks and gradually destroys the thyroid. Hashi's is the most common cause of hypothyroidism.
For non-autoimmune hypothyroidism a GP will generally wait until TSH reaches 10, where antibodies are raised this is positive for Hashi's and as long as TSH is over range at the same time as antibodies are raised then you should get a diagnosis and be started on Levothyroxine.
I would show these results to your GP, he may not like the fact that you have had private tests done and may not accept them, in which case invite him to do his own test to include antibodies. At primary level only TPO antibodies are likely to be done, Tg antibodies tend to only be tested at secondary level.
An over range TSH would be classed as "subclinical hypothyroidism" and guidelines suggest testing TPO antibodies - see:
Autoimmune thyroid disease is suspected — raised levels may suggest autoimmune primary hypothyroidism.
Do not arrange repeat testing of TPOAb.
A diagnosis of subclinical hypothyroidism is suspected — positive TPOAb can predict progression to overt hypothyroidism.
Do not arrange repeat testing of TPOAb.
So hopefully your GP will accept your Medichecks results, if not then hopefully he will do his own testing to include TPO antibodies and they come back raised along with a raised TSH.
Some general information about Hashi's:
Fluctuations in symptoms and test results are common with Hashi's.
Most doctors dismiss antibodies as being of no importance and know little or nothing about Hashi's and how it affects the patient, test results and symptoms. You need to read, learn, understand and help yourself where Hashi's is concerned.
Some members have found that adopting a strict gluten free diet can help, although there is no guarantee.
Gluten contains gliadin (a protein) which is thought to trigger autoimmune attacks so eliminating gluten can help reduce these attacks.
You don't need to be gluten sensitive or have Coeliac disease for a gluten free diet to help.
Supplementing with selenium l-selenomethionine 200mcg daily is said to help reduce the antibodies, as can keeping TSH suppressed.
Hashi's and gut absorption problems tend to go hand in hand and can very often result in low nutrient levels or deficiencies. It's essential to test Vit D, B12, Folate and Ferritin and address any problems. You are welcome to post these results, including reference ranges (plus units of measurement for Vit D and B12), for comment and suggestions for supplementing where necessary.
Wow, thanks for the very detailed reply. So much valuable information to go on.
I got my GP blood test results back a couple of weeks ago. Here are some values:
- Vitamin D = 156 nmol. My levels have been low for a very long time for many years, but the last 3 months I've been correcting that with high supplementation and my vitamin D levels are finally in the optimal range for the first time.
- B12 = 429 pg (normal 197-771)
- Serum Folate = 19.3 (normal 3-20)
- Ferritin wasn't tested but back in 2014 it was 86ug (normal 30-400)
- Vitamin D = 156 nmol. My levels have been low for a very long time for many years, but the last 3 months I've been correcting that with high supplementation and my vitamin D levels are finally in the optimal range for the first time.
You now need to maintain this level using a maintenance dose of D3 which will be lower than the dose you used to achieve this level.
The Vit D Society and Grassroots Health recommend a level of 100-150nmol/L, with a recent blog post on Grassroots Health mentioning a study which recommends over 125nmol/L.
It's trial and error to find this maintenance dose it may be 2000iu daily, maybe more or less, maybe less in summer than winter, so it's recommended to retest twice a year to keep within the recommended range. This can be done with a private fingerprick blood spot test with an NHS lab which offers this test to the general public:
Suggested times to test are end of October/beginning November to see what dose you may need for the winter, then around April/May because you may be able to make Vit D naturally from the sun during the summer so may need less.
Doctors don't know, because they're not taught much about nutrients, but there are important cofactors needed when taking D3. You will have to buy these yourself.
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc. 90-100mcg K2-MK7 is enough for up to 10,000iu D3.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking D3 as tablets/capsules/softgels, no necessity if using an oral spray.
For D3 I like Doctor's Best D3 softgels, they are an oil based very small softgel which contains just two ingredients - D3 and extra virgin olive oil, a good quality, nice clean supplement which is budget friendly. Some people like BetterYou oral spray but this contains a lot of excipients and works out more expensive.
For Vit K2-MK7 I like Vitabay or Vegavero brands which contain the correct form of K2-MK7 - the "All Trans" form rather than the "Cis" form. The All Trans form is the bioactive form, a bit like methylfolate is the bioactive form of folic acid. Both are German brands and can often be found on Amazon or Ebay but do go out of stock from time to time. If I can't get the 100mcg dose I buy the 200mcg dose and take alternate days. You can also buy direct from their websites.
If looking for a combined D3/K2 supplement, this one has 3,000iu D3 and 50mcg K2-MK7. The company has told me the K2-MK7 is the Trans form
Magnesium helps D3 to work. We need magnesium so that the body utilises D3, it's required to convert Vit D into it's active form, and large doses of D3 can induce depletion of magnesium. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking magnesium as tablets/capsules, no necessity if using topical forms of magnesium.
This is on the lowish side. According to an extract from the book, "Could it be B12?" by Sally M. Pacholok:
"We believe that the 'normal' serum B12 threshold needs to be raised from 200 pg/ml to at least 450 pg/ml because deficiencies begin to appear in the cerebrospinal fluid below 550".
"For brain and nervous system health and prevention of disease in older adults, serum B12 levels should be maintained near or above 1000 pg/ml."
- Serum Folate = 19.3 (normal 3-20)
Have you been supplementing with B Complex or a folate supplement?
- Ferritin wasn't tested but back in 2014 it was 86ug (normal 30-400)
Not relevant now I'm afraid. Ferritin is recommended to be half way through range so you'd be looking around 200 with your range. It's always useful to have an inflammation marker (eg CRP) tested at the same time as ferritin, this is because ferritin can be raised when inflammation or infection is present and this would show up with the inflammation marker test. Plus, of course, a full iron panel to include Serum Iron, Transferrin Saturation percentage, Total Iron Binding Capacity plus Ferritin is best as it gives the whole picture.
I've been taking a standard strength multi-vitamin everyday, but that's all.
I joined a vitamin D Facebook group a few months ago, and they were the people that guided me into corrected my vitamin D levels (my levels were at 36 nmol 3 months ago, and I've managed to get my levels to 156 nmol now). I'm aware of the co-factors to take too (Vitamin K2 and Magnesium). I have a problem taking magnesium orally due to tummy problems (even Bisglycinate), but found magnesium skin gel and it works really well for me, and actually helps my chronic insomnia too.
Good that the magnesium gel works for you, I can't stand the feel of it on my skin but do tolerate a small amount on my foot when I get cramp.
I've been taking a standard strength multi-vitamin everyday, but that's all.
Multi's aren't recommended here. They contain too little of anything to help low levels or deficiencies, contain things that compete with each other and should be taken at different times, tend to use the cheapest and least absorbable of active ingredients and often contain things it's important to test for first and only supplement if found to be needed, eg calcium, iron, iodine.
If it contains iron then this can affect absorption of everything else as iron needs to be taken 2 hours away from all other supplements and most medication, but 4 hours away from thyroid meds.
Iodine should not be supplemented unless tested and found to be deficient and then supplemented under the guidance of an experienced practioner. Iodine solution used to be used to threat hypERthyroidism before the current radioactive iodine treatment, so it can cause hypOthyroidism or make it worse. Also should not be taken when Hashi's is present.
Looks like you will get a hypo diagnosis based on recent tests....GP might want to do one more
I would stick my neck out and say that if your GP initiates levothyroxine treatment, starting dose 50mcg then things will improve.Testing should be repeated after 6/8 weeks to allow the hormone to settle into the system and the dose reviewed
Repeat the test/dose/ increase cycle until you feel well and labs reflect that.
You have worked on the essential nutrients.
Many find a gluten free diet helps with Hashi's ...there is no special medication.
We are advised not to use multi vitamin/ mineral tablets....best to take what you know you need and not what you do not!
Don't worry about the prospect of an hypo diagnosis...the majority of patients respond well to levo treatment and just get on with life. They are not here!!
Those of us here are in the minority and for various reasons do not respond well to levo
So, no need to be concerned... unless you don't respond well....
and even then most things can be overcome with appropriate medication
I have a rare thyroid condition which medics had no idea how to treat and which left me very unwell....this forum helped me find those elusive answers!
The collective thyroid knowledge of members far exceeds that of most medics so you are in a safe place here.
Great advice, thanks. The only thing that worries me is that my biggest health concern is chronic insomnia (all my life). My mind is just so over active in bed. Would taking medication for an under active thyroid make that worse?
There's no history of auto-immune disease in my family.
I got my GP blood test results back a couple of weeks ago. Here are some values:
- Vitamin D = 156 nmol. My levels have been low for a very long time for many years, but the last 3 months I've been correcting that with high supplementation and my vitamin D levels are finally in the optimal range for the first time.
- B12 = 429 pg (normal 197-771)
- Serum Folate = 19.3 (normal 3-20)
- Ferritin wasn't tested but back in 2014 it was 86ug (normal 30-400)
Taking a separate vitamin D and separate good quality vitamin B complex that has folate in (not folic acid)
Recommended brand- Thorne basic B
Also remember to stop taking vitamin B complex or any supplements that contain biotin a week before all blood tests as biotin can falsely affect test results (it’s used in many lab tests)
Never iron unless tested full iron panel test for anaemia and found to be low. Can have high iron and low ferritin or vice versa.
Hi Mr_PBS .... i'm assuming you don't already have a diagnosis of hypothyroid, and are not already prescribed Levothyroxine (replacement T4) ?
These results show you are developing Autoimmune Hypothyroidism. (commonly called Hashimoto's)
You should show these results to to your GP.
He will probably wish to do his own NHS testing to confirm TSH and fT4 , and (depending on his results and your symptoms ).....
If your T4 is below range in his test, he may wish to either start you on levothyroxine straight away .. but if your fT4 is in range in his test , he will probably need to wait 3 months for a repeat test of TSH and fT4 results.
The NHS guidelines say they need "two 'over range' TSH results 3 months apart + symptoms" , before they are allowed to prescribe replacement T4 hormone (levothyroxine)
Because your TSH isn't very high (yet) if your fT4 is in range in their test , he may not want to prescribe yet.
But your high TPOab (thyroid peroxidase antibodies) show you are very likely to become more hypothyroid over time (higher TSH / lower fT4) , and will need thyroid hormone replacement eventually .
They will take the raised TPOab antibodies into account, and any symptoms of hypothyroidsm (feeling cold / slow / constipated / gaining weight/ depression/ loosing outer third of eyebrows / dry skin / course hair/ deeper voice/raised cholesterol / slower heart rate etc. etc .etc .. there are hundreds of symptoms of hypothyroidism because thyroid hormones control the function of nearly all the cells in your body .. when you aren't getting enough thyroid hormone T4/T3 .. your whole body, (and brain) gradually 'slows down'.
TSH (Thyroid Stimulating Hormone) is a massage from your pituitary to your thyroid gland asking it to produce more thyroid hormones (T4/ T3) ~ higher TSH = "T4 is too low , make more please"
If the thyroid is slowly being damaged by the immune system, then it becomes unable to make enough T4 /T3... so the T4 level gradually goes down . and the TSH gradually goes up... and will keep going higher, as T4 get's lower.
The high antibodies, particularly the TPOab (thyroid peroxidase antibodies) are how the GP knows that the reason for your low T4 is autoimmune damage, and not some other reason .
Fewer men than women get autoimmune hypothyroidism , but there are quite a few males with it on here... so you are unusual , but not alone .
My GP has already done one blood test for my thyroid & I got the results about 2 weeks ago. My GP was a bit concerned about the result and asked me to do another test in 2 months time. That's why i decided to buy a Medichecks test for my own curiosity about the possibility of auto-immune problems.
These were the values for my thyroid from my GP's test 2 weeks ago:
ah ... right . So if your TSH is still over range in his second test, then he would probably have done the TPOab then, to see if that was the reason for the high TSH remaining high/ low end T4 .. so you've saved him the bother .
Autoimmune disease is by far the most common reason for developing hypothyroidism , so they don't always bother since it doesn't affect the treatment options ... it just gives them more confidence that it's going to be needed anyway at some point .. so it allows them to prescribe earlier with more confidence. But since thyroid hormone replacement is a life long treatment ,they need to make sure it isn't just a temporary rise in TSH / lower fT4 that could be due to something temporary and would right itself. ( hence the 'repeat in 2/3 months' bit )
But your TSH at nearly 6 ,and your fT4 crawling along the bottom, coupled with your high TPOb mean there is about '0' chance this is going to get better by itself.... GP still probably has to wait for 'his' second test results though .
When you go for you repeat test at GP .. make sure you get an (earlyish) morning appointment for the blood draw ( even if this means waiting a few more weeks to get one)
TSH has a circadian rhythm .. it is highest middle of the night , and falls to it's lowest around 1-3pm ish .. then slowly rises again)...... so if you go for a blood test at the lowest part of the day, your TSH will look like it's got 'better' (lower) .. and if it was only just over the range on that test (like 4.999) this could stop/ delay the GP prescribing .
NHS will tell you you can have the TSH test at any time of day.. conveniently ignoring the circadian rhythm ,and therefore delaying the diagnosis of a lot of 'borderline' patients who happen to go for TSH test in the afternoon .... they won't accept you saying 'my TSH needs to be tested at 9 am'.... but really it is a good idea to have it done early am ... and also it is a good idea to have all your future TSH test done at a similar time for consistency , so you can monitor any changes properly.
I always just tell the receptionist 'i cant get here after 9 .30 am due to work commitments ' cos it's not worth the argument with the receptionist who's computer will undoubtedly say "TSH can be taken any time of day"
Great advice. Thank you. The only thing that worries me about taking thyroid medication is even if i have an under active thyroid i also have an over active mind, hence the chronic insomnia. When I'm in bed trying to sleep i cannot get myself to "shut up", lol, just thought after thought after thought speeding through my mind.
Hi Mr PSB. It sounds like you suffer from chronic anxiety which is affecting your sleep. You probably ruminate a lot and worry about things, trying to find answers to everything? It will keep you from getting to sleep and it disturbs your sleep which is exhausting. It's a classic symptom of anxiety.
Yep, that sounds about right. I have quite bad OCD too. All my life i've had a loud high pitched tone in my head too. It's as loud as my thoughts. It makes it hard to sleep. I've had it as far back as i can remember (child). It's really strange because as soon as i notice it it actually gets louder.
Hi. Given your description I'm thinking it's likely something you were born with, the way you're wired so to speak, if you've always been this way. If your thyroid is now causing issues that could well make it worse. In that case addressing the thyroid issue might improve things but if the chronic anxiety/OCD has a genetic cause separate to thyroid, then it's unlikely to be completely cured by thyroid medication. It can be helped though if you can find what works for you.
Something i've just realised is that i took the Medichecks finger prick test at about 2am. I do have a weird body clock though as I normally go to bed at about 4am. Having said that, the Medichecks results were quite similar to the test my GP done for me a couple of weeks earlier at about midday. The main purpose of the Medichecks test was to test for the antibodies.
just a quick reply . cos i don't have insomnia any more (lucky me) it's crap isnt it , been there, done that bought the T-shirt ....and the brain that won't shut up ..but im better now . No.... taking levo won't make your brain go faster at night ... in fact it might well improve your insomnia . seem to remember one of the admins on here Helvella (also male) , had insomnia before got prescribed levo.. i'm sure he said it was the first thing that improved ... got to go and let the cat out and go to sleep now
We need good thyroid levels for good restorative sleep
Likely your insomnia will improve once you get established on levothyroxine
It does take several weeks/months to build up to right levels …..Not a quick fix like an aspirin
If your GP has tested cholesterol…..high cholesterol cholesterol is also linked to being hypothyroid and will improve as levothyroxine dose is increased
How interesting. Thank you. The thing that is annoying me now is that I've been going to various doctors for a long time because of my chronic insomnia but none of them ever considered it may be because of thyroid problems.
This is my first post/reply here too, like you I am male but aged 62 and have the same issue where I tested with Medichecks and had to prove my health condition existed when my doctor thought it only needed 25mcg levothyroxine even though I recovered from serious Graves disease 27 years ago!
After many months and two endo's I am now on 75mcg levo and 2 x 20mcg liothyronine daily which inhibits my TSH and T4 levels but helps greatly with my T3 levels as conversion is an issue with me.
One thing I would say is with autoimmune thyroid disease it can come with other autoimmune disease where your body is attacking itself like diabetes, vitiligo, alopecia areata, anti-gastric parietal cell antibodies to name but a few so you could have a fight on your hands to feel better sorry to say and you need to make sure your vitamin levels are all well into the green so test them also as described by SeasideSusie.
I'm assuming that your multi-vitamin/multi-mineral contained folic acid. I'm always dubious when people quote high levels for folate.
Folic acid is not a natural form of folate - it was developed in 1943. The body has to convert folic acid to methylfolate before it can be used. And surprise, surprise, a lot of people can't do the conversion or they only do it very slowly. So your high level for folate is likely to be a high level of unmetabolised folic acid.
What you need instead is something the body can use without further conversion, such as methylfolate which can be bought on sites selling supplements.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.