Firstly, thank you so much for everyone sharing their thyroid stories and for the amazing feedback & support given by the community. You have all provided much needed reassurance and confidence, especially when facing GPs.
I've been struggling with hypothyroid symptoms for what I believe has been around the past 3 years, perhaps even longer, with them getting increasingly worse over the past 12 months, over which time I've had various blood tests.
I've discussed the results of tests ordered by my GP with them while I've been living in Leeds, with one referring me to the endocrinologist who refused to see me, and the other first suggesting I may be suffering from subclinical hypothyroidism.
After seeing the result of a requested antibody test, the same GP then said it couldn't be subclinical hypothyroidism and refused my request for a thyroxine trial as, and I quote, "I don't want to make you hyperthyroid" with no more advice then given.
Sufficed to say, I wasn't all that happy so I went ahead and ordered the Thyroid Check PLUS TWELVE (With Reverse T3) test from Blue Horizons.
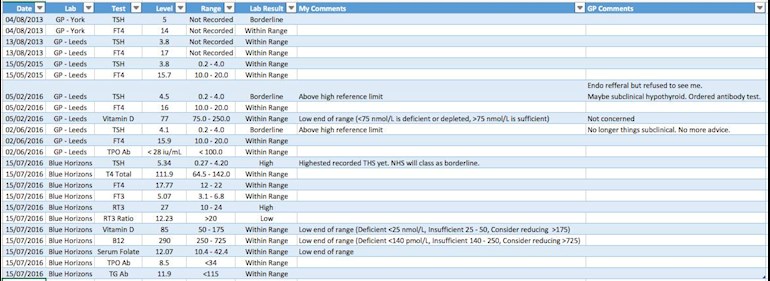
The results, as I understand them, still point to subclinical hypothyroidism but with the high RT3, low RT3 ratio, and vitamin & mineral levels being on the low end of the normal range, I'm worried that there's more going on here.
I would really appreciate any and all help surrounding interpreting my test results with possible insights into adrenal fatigue and pituitary issues.
The symptoms did appear to get much worse during a stressful project in work but they were present before then and haven't eased off now that I'm under less stress, although I understand that stress doesn't just disappear overnight.
I've added a screenshot of a test results spreadsheet that I keep track of and I'll try to add another photo if I can with a list of my symptoms.
Other useful information might be that my mother was diagnosed with hypothyroidism (unfortunately I don't have her test results) and my sister suspects that she might be.
Many thanks.
Written by
abunnyuk
To view profiles and participate in discussions please or .
David, I think the reason you haven't had any replies, is that your results are too difficult to read. The writing is very small, and goes blurry if you enlarge it. And, then, the way it's laid out makes it very difficult to understand. All I could really see was that your TSH goes up and down a bit. Did you have all the tests done at the same time and fasting? If not, you can't compare them, I'm afraid.
abunnyuk As far as your vitamin and minerals are concerned, you could do with supplementing all round.
B12 - 290 - way too low. Supplement with Jarrows or Solgar sublingual methylcobalamin lozenges 5000mcg. The Pernicious Anaemia Society recommends 1000. Once at optimal levels a maintenance dose of 1000mcg will be fine. You can't overdose on B vitamins, any excess is pee'd out. If you take B12 you need a B Complex to balance the B Vits (see Folate).
Folate - 12.07 (10-4-42.4) - way too low. Folate should be at least half way through range so about 26+ is where it should be. To raise folate supplement with a good B Complex (Thorne Basic B or Jarrows B Right), both contain 400mcg methylfolate. Thorne Basic B got mine up from bottom of range to top of range is 2.5 months.
Vit D - 85 - not too bad but 100+ is better. I'd add in a D3 supplement, something like 2,000iu per day. When supplementing with Vit D you need to take K2. Vit D aids absorption of calcium and K2 directs the calcium to bones and teeth rather than soft tissues. Look for K2-MK7.
Ferritin - you haven't listed this, it would be included with a BH Thyroid Plus 12. If it isn't at least half way through range you will need an iron supplement which should be taken with 1000mg Vit C to aid absorption and help prevent constipation.
Getting optimal levels of vits and mins may help you feel better generally.
Your results this year show a constantly over range TSH and it's a fair bit higher now than it was a couple of months ago. With your FT4 'normal' and not varying greatly, and your FT3 'normal' - I'm wondering why your GP has now discounted subclinical hypothyroidism. According to BMJ Best Practice bestpractice.bmj.com/best-p...
High TSH - associated with a normal FT4 and/or FT3
•Subclinical (or mild) hypothyroidism occurs when TSH is above reference range with a normal FT4 and FT3. The risk of progression to overt hypothyroidism is 2% to 5% per year. [43] The risk is higher in patients with positive TPOAb. [44] The decision to treat these patients is controversial. Generally, thyroxine replacement is not recommended when TSH is below 10 mIU/L. [45] TSH and FT4 should be repeated at 6- to 12-month intervals to monitor for improvement or worsening in thyroid status in untreated patients. [43]
Maybe you could point this out to your GP and ask why he is no longer considering subclinical hypo.
I don't know anything about a high rT3 in a non-medicated hypo patient I'm afraid, I only know a bit about what would be done with a patient already on medication.
As thyroid and adrenals are linked, and you have mentioned adrenals, you could get the Genova 24 hour saliva adrenal stress test, it all helps build up a picture. Details of how to order and how to receive results are here thyroiduk.org.uk/tuk/testin... and if you check the pdf test list you will see the test you need is END01
abunnyuk With your most recent results your FT4 is 57% through it's range, so that is mid range rather than low. Your FT3 is 53% through it's range so again mid range. You are obviously converting T4 (the pro hormone) into T3 (the active hormone) quite well as the ratio of FT4:FT3 should be 4:1 or less for good conversion and yours is 3.5 : 1.
[It's a shame we're not given thyroid tests as a matter of course when well, it would be very useful to know where our individual 'normal/optimal' is and then it would be so much easier to diagnose and treat thyroid problems if they occur.]
Even though your free T levels are over 50% through the range and are 'normal' in the eyes of the doctor, he (nor you for that matter) doesn't know whether that's your normal but your symptoms are indicating you're not well with those levels. Obviously with a high, and rising, TSH there's something not right but it looks very much like your doctor is going to stick to the guidelines and do nothing until your TSH reaches the magic number 10 and he can then pronounce you hypothyroid.
There is a reason for your high reverse T3 and I don't really know much about that. A very quick Google ('cos I really ought to go to bed but I've just thought of it ) of 'high reverse T3 in euthyroid patients' brings up some articles that might be worth reading so you could research that.
This is an article on high reverse T3 but in hypo patients but it's worth a read just in case it gives you any clues stopthethyroidmadness.com/r...
And the only other thing I can think of is if you are on any medication for anything that might be connected to your issues. I don't know if anything would be, it's just a thought.
It might be an idea to start a new thread with the title something like 'High rT3, over range TSH, normal free Ts" to attract the attention of anyone who has knowledge of rT3 issues.
I have just tested high in rT3, with low T3 and have been looking for info.
This is from "tired thyroid" & gives lots of causes for rT3 - half a dozen of which could apply to me. See if it helps with furthering your understanding... it's all so complicated. .
There are refs on the web site:
Reverse T3’s role in the body
Normal, healthy people produce reverse T3, it is not poison, and it is a normal pathway for the breakdown of T4. It is actually abnormal to have no reverse T3! [7]
One purpose of reverse T3 is to reduce metabolism, to prevent starvation in cases of famine. Anyone on a severe caloric restriction diet will reach a weight plateau at some point because reverse T3 naturally rises in this condition. [8]
Marathon athletes can also have high reverse T3 levels for the same reason—the body is trying to conserve energy to prevent starvation. People on strict diets who overexercise should expect higher reverse T3 levels. [9]
Studies show that there are many other causes of high reverse T3 levels:
aging
burns/thermal injury
chemical exposure
cold exposure
chronic alcohol intake
free radical load
hemorrhagic shock (often from severe blood loss)
insulin-dependent diabetes mellitus
liver disease
kidney disease
severe or systemic illness
severe injury
stress
surgery
toxic metal exposure
certain drugs like amiodarone and beta blockers
and high cortisol. [10,11,12,13]
It’s much healthier to address and correct the conditions just listed, than to take T3 only. Diabetics typically have high reverse T3 levels that drop once their glucose is controlled. [14]
Reverse T3 levels can appear high in someone whose liver is not healthy, because reverse T3 is processed and eliminated in the liver. [4,5] There are anecdotal accounts from people who have a suboptimal reverse T3 ratio, with both FT3 and reverse T3 over mid-range, but who feel fine. As long as the FT3 was optimal for them, it didn’t matter what the reverse T3 level was..."
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

") ) of 'high reverse T3 in euthyroid patients' brings up some articles that might be worth reading so you could research that.
) of 'high reverse T3 in euthyroid patients' brings up some articles that might be worth reading so you could research that.