This subject is coming over and over into surface, so I decided to start a specific thread as I got bored in writing the same things over and over again:
Post RP patients with a rising PSA are discouraged to take a PSMA PET/CT imaging before deciding on sRT, on the grounds that it will detect "nothing" at their low PSA value, usually in the range of 0.1 to 0.2.
First important comment is that the pre-test PSA value is not the only and _certainly_ not the best metric for this. PSADT is more important, but the clumsy way by which PSADT is usually derived leads us to better leave it out of this discussion. A brief explanation to this is that PSADT is the mathematical/numerical first derivative of PSA. Elementary knowledge of math and their application to measurements, indicates that the accuracy of the first derivative of any variable is an order of magnitude inferior compared to that of the variable itself. Taking 20% as a ballpark for the PSA measurement accuracy, the thus derived PSADT mounts up to 200%. There are ways to do better for the former and consequently the latter, but this is not our current subject.
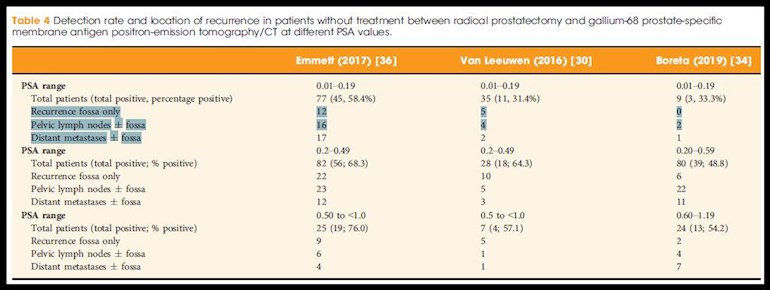
Now lets have a look at Table 4 of the paper entitled:
"Use of gallium-68 prostate-specific membrane antigen positron-emission tomography for detecting lymph node metastases in primary and recurrent prostate cancer and location of recurrence after radical prostatectomy: an overview of the current literature" (2019)
Three studies for the PSA range of 0.01 to 0.20 (cumulatively 121 cases) are recorded. Out of them 59 cases (48.8%) led to a positive detection. The second comment here is that the radio tracer used in all three studies was 68Ga while today there are its 18F counterparts that are considered of being more sensitive in the lower PSA scale. Also, since 2 years ago there are digital PET scanners that are equipped with more sensitive detectors. Consequently, this 48.8%, considered as "nothing" by the naysayers, is a conservative figure by today's standards.
But the most important part of this discussion comes from the break-down of the location of the detected lesions:
Recurrence fossa only: 17 cases -> 14%
Pelvic lymph nodes +/- fossa: 22 cases -> 18%
Distant metastases +/- fossa: 20 cases -> 16.5%
Now, if we make the assumption that a similar break down characterizes all the lesions that due to their low concentration (not size < 5 mm - another grossly silly statement) that evaded detection, it is clear to see why sRT has a ~65% roof in success score. The remaining ~35% failed because the cancer was distant or distant as well to the irradiated field.
Lastly, there is the ultimately silly argument: Why take the test if it is not going to change your treatment plan. Because, there is a myriad of studies concluding that after a positive PSMA detection 1/3 to 1/2 of all irradiation plans were modified slightly or heavily to the limit of excluding this 16.5% (distant metastases) as bringing nothing but late toxicities.
The only difficult thing about it is to find a competent RO among the sea of incompetence that wants to rule.
Written by
Justfor_
To view profiles and participate in discussions please or .
~6 months ago I asked my MO for a PSMA scan. She said that my PSA was too low (zero) and that the insurance companies would deny it unless my PSA was over 0.3. I replied, "0.3? I can do that". She didn't really understand what I meant (my wife was with me and she looked at me and laughed - she knew that I wasn't joking).
I might readdress this. I'm doing BAT+ and on the high T phase, my PSA goes well above 0.3. So far it has been undetectable a month into the low T phase. I can easily get her proof of PSA > 0.3 (last phase I went as high as 0.71).
If you really want a PSMA test and need your PSA to be >0.3 to get one, maybe a few applications of Androgel will get you there?
That is really high. What type of T are you using?
I use Androgel and propionate, and soon I'm going to try oral undecanoate. Recently I tested Androgel efficacy so I applied 300 mg and had my tT measured 4 hours afterward to get the approximate max. It was 4971 ng/dl, fT was 181 ng/dl and bioT was 4481 ng/dl.
My PSA when I got the T up to 1800 measured 0.2-0.3 with corresponding lower levels of fT and bT (SHBG and albumin haven't changed much). I had my PSA measured at the same time as the 4971 T test and it was 0.71. I hope that it was due to androgen stimulated PSA increases NIH estimates the PSA increase from T can be 7x or higher. The graph below is from the patient's guide to BAT by Denmeade. Cancer can be regressing yet PSA increases. My MO discussed that with me. Even my urologist at Mayo hinted at it years ago.
That said, I wouldn't advise doing SPT unless you really like that particular QoL and are willing to take risks to get it. If you want to go the insurance route you might need to find a more sympathetic MO. My MO told me that even with undetectable PSAs she would authorize the test for me. But she told me that my insurance would not pay and that there was "nothing to find" in my case. Still, it would be nice to get a baseline so I might ask her again. And now I have the required insurance company proof.
Thanks for letting me know about my grammatical error. I wrote that at 3 AM my time so I'm surprised that it was in English and was somewhat legible.
Thanks for the graph, I will study it to see if there is something compatible with my personal case as, in the past before starting Bicalutamide, I had tried the correlation of PSA to tT, even that of the rate of rise of PSA to tT with R^2 coefficients disappointingly low.
I use two labs. The first specifies the method for tT measurement as: Electrochemiluminescence / ECLIA. After starting Bicalutamide, reported values are more volatile, spanning from 2250 to 3090.
The other lab, doesn't specify the method used but reports lower and more tightly spaced values (1650-1700) for the same period.
My regards to your MO. She got a seat in my non-silly doctors list. Kudos to her!
That's right. I forgot that you were on Caso. That will cause your serum tT to go high. Do you have fT and bioT measurements from pre and post-Casodex? We could maybe see something from the individual levels (activity).
The graph is in this doc:
1. Bipolar androgen therapy (BAT): A patient’s guide - Denmeade - - The Prostate - Wiley Online Library
Even if r-squared was better it's a moving target. Be hard to get a good correlation without hundreds of data points and maybe that wouldn't be good enough. My self stats are problematic but I think that they are infinitely better than nothing. And many times they are better than what we get in trials. People have various responses. Even the experts know this and sometimes scratch their heads and look for clues. Yet people frequently fall into the trap of thinking that everyone is average and acts the same. Wrong. Why did I respond so well to high testosterone for 2 years? Why did my PSA never bounce high after I started?
My Drs wanted a Axumin scan which was refused by insurance company but my Drs said it wouldn'tchange treatment. My high PSA wasn't presenting a clear source of PSA on CT and bone scan. My RO tried to identify where it was with a biopsy and then an MRI to determine if I would get the full RT or just a boost to the gland and start systemic treatment. So clearly it would have changed my treatment just not my MO's which I saw first. I received the full RT into abdomen. If I had been diagnosed now PSMA Pet would have been approved per my MO.
It takes time for the tidal wave to influx the shore. Patient is sine qua non (εκ των ων ουκ άνευ - as per the Greek version that predates the Latin - dedicated to my friend J-O-H-N)
It is easy to make your PSA goes up. One week before do the PSA test, you take Vitamin B12 and do cycling half an hour everyday.
I was told that I needed to experience three rising PSA scores, presumably at 3 or 4 month intervals, to qualify for an Axumin scan, which I received. The scan showed no activity. Last PSA reading was 1.8. I'm not on ADT.
Back to your original post, are you suggesting that in any BCR, one has sRT (either/both general pelvic area/nodes and any other identifiable mets) and something for the possible distance mets floating around even if 68Ga PSMA scan shows nothing (like mine did)? Chemo? I think I heard about one doc recommending that. Kwon?
No, I say that blind sRT has a higher rate of failure and since it is not without side effects and late toxicities a PSMA scan ( positive or negative doesn't matter - both provide useful information) improves the gain to cost ratio.
The following is only for those interested in the math behind PSADT. My TL;DR for anyone else is that I respectfully disagree that PSADT is generally an order of magnitude less accurate than the PSA measurement. It’s possible, but it’s not necessarily true.
The PSADT precision is a function of the data that is input into its calculation — more PSA data points that are given over “closer” periods of time ==> more precision. If you have only a few PSA measurements done over long periods of time, then it’s easy to imagine order of magnitude (or worse) levels of error for PSADT.
Please read no further if math bores you. My impression is that Justfor_ has some math savvy, and I LOVE that sh*t, so I’d like to dig into that with him.
————————————————————————————————————————————
Justfor_, the 1st derivative of PSA would be PSA velocity, much the same as a physical velocity is the 1st derivative of position. So PSADT is a different thing; it is in units of months, not ng/ml/month (as would be true for the 1st time derivative of ng/ml).
…PSADT is calculated qualitatively as follows: “…the natural logarithm of 2 divided by the slope obtained from fitting a linear regression of the natural log of PSA on time.” From a source I found long ago but don’t exactly recall, I found this (rough) formula that seems to match up with this:
(ln(2)*Δt)/(ln(PSA_final/PSA_initial)
…where the Δt is the amount of time in months elapsed between measurement of an initial PSA and a final one. Importantly, please note that this formula uses only two PSA measurements — so our “linear regression” precision is a function of the “proximity” of the points in time (closer = better fit = more precision).
So even though the nomogram and this formula might match up for two PSA points, the precision of the PSADT would seem to diminish with wider time intervals between initial and final PSA values, i.e. the linear fit would get further and further away from the actual “function” curve that defines the PSA trajectory. Do you agree?
There is likely a more sophisticated formula that can account for an arbitrary # of PSA measurements…and this is what I mean by my opening statement about more PSA points at closer intervals = better precision PSADT.
In either event, as an example to test drive my “rough” formula — if you have this situation:
Date 5/28/2021 PSA 5.76
Date 7/30/2021 PSA 7.5
…and you plug these numbers into the MSKCC nomogram at mskcc.org/nomograms/prostat..., you’ll get doubling time of 5.4 months.
You can likewise use my given natural log-based formula in an online calculator (you can even just ask Google). Here’s how I use the formula:
— for the given dates, you have 63 days, if I did that correctly…
— the next hurdle is what value to use for the Δt. Here we need to define “month”...I’ll use 365/12 to get around the ambiguity in this definition (is it 28 days? 30? 31? etc)….
— with this, we can calculate Δt using 63/(365/12):
(ln(2)*(63/(365/12)))/(ln(7.5/5.76))
This calculation gives us 5.43, which rounds down to match with the nomogram. So we have at least some empirical confidence level that the formula is useful, possibly “correct”, for an initial and final PSA value. Again, it’s most useful (since it’s most precise) if the time interval is a “small” one.
Justfor_ , as an aside out of my own curiosity:
…you’ve also stated that “the accuracy of the first derivative of any variable is an order of magnitude inferior compared to that of the variable itself.” Could you point me to a reference that elaborates on this?
I am aware of differential equation techniques where we can approximate derivatives, and these approximations can indeed have less than exact precision (I wouldn’t be surprised if in some cases an order of magnitude of error).
But there is a formulation as given by Newton and Leibniz that mathematically (i.e., as far as I can tell, “exactly”) determines the limit of a given function, i.e. it gives us exact results for any order of derivative (1st, 2nd, etc). Using the context of particle motion, the particle velocity can be calculated exactly at any given point of time if we know the function defining its motion.
Anyway — phew! Thanks for indulging me. Most importantly of course, I wish you the best of luck in your fight with this cancer, and in finding the right doctors for your situation.
Thanks lokibear for taking the time to write such a long post.
Firstly, you are correct that PSA velocity is by definition the first derivative of PSA.
PSADT is also expressing the PSA velocity but in a very specific way incorporating the log function as it is thought (which is not always true) that PSA follows an exponential rise.
Secondly, I will pass giving you any links regarding the accuracy of the derivative as I am a practical person and always prefer to put my gray cells in motion to canned knowledge. Instead, I will give you a real world example that will also make it more easy to follow by the lay members of this site:
Take for example a small child that has a height of one meter. Our measuring device has an accuracy of +/- 1 cm (+/- 1% measurement accuracy in this case). One year later this child has grew taller by 5 cm to 1.05 m (velocity = 5 cm/year). We measure again with the same measuring device and try to derive the growth rate:
There are 2 extreme cases:
a) 99cm at first measurement, 106 cm at second -> 7 cm gained during one year
b) 101 cm at first measurement, 104 cm at second -> 3 cm gained during one year
Consequently, we can end up with a +/- 2 cm error on the 5 cm/year value (+/- 40% measurement accuracy). QED.
Lastly, since you sound pedantic about it, it is true that for PSADT this error amplification will be less than the linear example I just gave and this is due to the compression that the log function introduces. I leave it to you to try some numbers, following the methodology I showed above, with the online calculator you mentioned.
Very nice example, and your point is taken. My points were only that there is no inherent order of magnitude error in the 1st derivative, and that PSADT is not calculus-based regardless.
Obviously, if the input (as per your example) has inherent error, than of course anything derived from that will have a +/- built into it. I was referring to the use of calculus with known well-defined functions.
Our PSADT, of course, cannot be analyzed that way (though, I’ve tried, with limited success).
Perhaps the only relevant piece of this, wrt our forum: do you really believe there is a 20% ballpark error built-in to PSA measurements? That would be rather disturbing.
We agree on all of the above accounts. The 20% I got it from a FDA approval document for one assay/analyzer family combo. It is referenced as "Interlab". Different labs may have assays of different batch numbers, analyzers with newer or older heads, different calibration and maintenance protocols and most importantly different reporting policies. The latter is very important at the lower PSA scale where the quantisation or rounding error is by itself the most important component. This error at PSA values inferior to 0.06, for reporting to two decimal places, is by itself 20% or more. I once had a chat with the responsible person of one lab who told me that they can go to 3 digital places but they wouldn't report it.
On the contrary, you wrote the most appropriate word "servo". Our body has, no-one knows how many, servo loops. I take Bicalutamide and the T shoots up. Why? Because the "sensor" measures low and signals "produce more" until saturation oçcures.
In Australia, the bulk of RP recurrent patients have PSMA PET/CT imaging before the start of salvage RT. On the flip side, in Belgium, blind RT is still business as usual.
This post addresses an important and nuanced discussion regarding the role of PSMA PET/CT imaging in post-radical prostatectomy (RP) patients with a rising PSA. Here's a breakdown of the key points and insights from the thread:
1. Discouraging Early PSMA PET/CT
Many clinicians argue against PSMA PET/CT imaging at low PSA levels (0.1–0.2) due to the belief that detection rates are too low.
However, this view is challenged, emphasizing that metrics like PSA doubling time (PSADT) are more relevant for decision-making than absolute PSA values.
The criticism of PSADT's unreliability (due to inaccuracies in PSA measurement and derived calculations) highlights the need for better tools or direct imaging.
---
2. Evidence Supporting Early Detection
The referenced Table 4 from the study shows detection rates for PSA values between 0.01–0.2 using Gallium-68 (68Ga) PSMA PET/CT:
Detection rate: 48.8% (conservative by today’s standards due to advancements in tracers and digital PET scanners).
This challenges the "detects nothing" argument often used to discourage early imaging.
Breakdown of Lesion Locations:
Recurrence in the fossa only: 14%
Pelvic lymph nodes (± fossa): 18%
Distant metastases (± fossa): 16.5%
This distribution underscores why salvage radiotherapy (sRT) has a ~65% success rate ceiling—the remainder likely fail due to undetected or untreatable distant disease.
---
3. Why Imaging Still Matters
Studies show that 1/3 to 1/2 of irradiation plans are adjusted based on positive PSMA imaging findings.
Early PSMA PET/CT can help refine the sRT field, targeting local recurrence, pelvic nodes, or excluding distant metastases. This tailored approach minimizes unnecessary toxicities while improving success rates.
---
4. Challenges in Clinical Practice
The need for skilled radiation oncologists (ROs) is emphasized, as some professionals may dismiss these tools or fail to adjust plans appropriately.
The thread suggests a lack of uniformity in expertise and adoption of advanced imaging, creating gaps in optimal patient care.
---
Conclusion:
This thread advocates for incorporating PSMA PET/CT imaging earlier in the decision-making process for post-RP patients with rising PSA, even at low levels. It highlights:
The inadequacy of relying solely on pre-test PSA values.
The potential for newer technologies (e.g., 18F tracers, digital PET scanners) to improve detection rates.
The need for individualized treatment plans informed by imaging findings to maximize sRT success and minimize toxicities.
Would you like further elaboration on any of these points or related studies?
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.