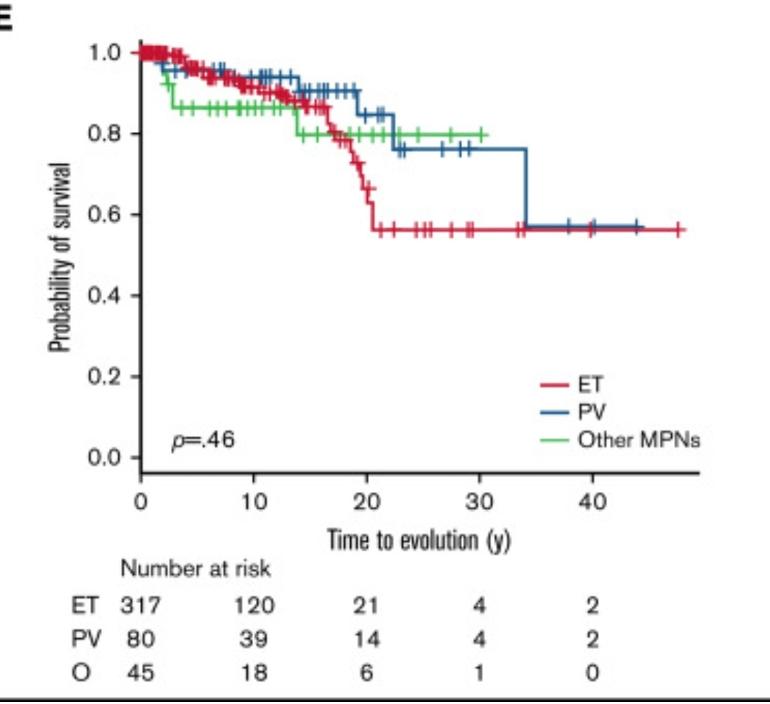
This study (link below), is from a young cohort of MPN patients. If you read the study, it says that 7.3% progressed to MF during the duration of the follow up.
But in the graph, it looks that this percentage is really higher during these 40 years or more specifically at 20 years. Why?
Does this mean that if someone has ET for 40 years has 40% (and more) probability/chances of progression??
I think so. Longer the disease , overproduction of blood cells for loner time may adversely affect the health of bone marrow leading to scarring and fibrosis.
There is the “1% per year” estimate that I’ve seen referenced many times. The risk of progression, generally speaking, seems to increase by about 1% per year. After 10 years, about 10% seem to progress. After 30 years, about 30% seem to progress. The data in this graph seems to somewhat agree with this.
Its general conclusion is prognosis for younger (under 25) is worse than previously found.
"Rates of thrombotic events and transformation were higher than expected compared with the previous literature."
Splenomegaly and Jak2 mutation (vs CALR, triple neg) were also negative prognostics.
"with splenomegaly as a novel risk factor for transformation in essential thrombocythemia (ET) (P= .000)" This P value I believe means the result was very statistically signif. (I've never seen a 0 before)
Note in Fig. 3 how few patients were at the longest times. This is also indicated I think by the long straight lines that show in later years. So the 30 + year results have few patients for reference.
They also seem to suggest bleeding is a higher risk in this group than clotting.
"these ...findings and would support control of thrombocytosis even in young patients to reduce bleeding risk" and "classical management with low-dose aspirin to prevent thrombosis should perhaps be questioned in this specific population"
This statement is not a good result, suggesting, at least in younger cohorts, that treatments did not help as much as they expected:
"We observed a high disease burden, with incidences of thrombotic events and transformations higher than previously reported in this population even though many patients were being treated with cytoreductive agents"
but "physicians did not apply ELN recommendations where interferon is the recommended first line therapy in patients aged <60 years old"
So maybe with higher use of IFN they would have seen a better result.
I was at the recent zoom webinar about ET from Guys abd the message came over that very few people progress. I find that hopeful as I’ve had ET for about 25 years.
That’s the message I’ve had repeatedly from haematologists. Some of these studies could be confounded by the number of years the subjects went undiagnosed, and more recently, someone posted about non-adherence to treatment, which has a bearing on progression. Then there’s the question of people being classified as ‘ET’ before ‘pre-fibrotic MF’ was found to be a separate disease entity. These are just my musings, though. And finally, there is the renaissance of IFN, which I’m sure we’ll discover has a disease-modifying effect by reducing the malignant clone, along with the mountain of MPN research into even better drugs that should improve our prognoses.
interesting paper, I skimmed it and two things stand out
1. It was 1990 to 2019, treatment has improved a lot since 1990 and very likely to improve rapidly soon, hopefully
2. Unfortunately most of us I assume are not young adults so maybe less relevant.
From various stats and conferences I’ve been to transformation to MF is roughly 10% at ten years and 15% at 15 years and so on. That should be read perhaps as 90% won’t at 10 years and 85% at 15 years won’t. That’s quite good percentages. That is also historical data so should improve going forward hopefully😀
i am a young MPN patient and i have ET since 17 years old. Now 39. So 10% at 10 years and 20% at 20 years, is very much. This means that by age 60 i will have ET for 40 years so 40%. It freaks me out.
Could @Mazcd clarify this for us through prof. Harisson?
sorry the intention is not to freak you out as you put it, its important to remember this is historic info ie its based on what happened going back decades. Also by the time your 60 ie in 21 years time treatments and will be wildly different and I would be surprised if there is not a cure long before then.
the fact that is historic info (cohort), doesn't mean that something has changed, cause no treatment until now has a real impact on disease progression.
Not then, not now. Maybe IFN, but has no strong clues yet
It's really about perception of risk. Even if these statistics are completely accurate (and it's always more complicated than that), you would still be in the majority who don't progress. In twenty years treatments will have improved.
Suppose that you progress - you would be treated for MF, which is not the end of the world. If you needed an SCT, they are improving all the time.
Cross each bridge if and when you come to it. And please get help for your extreme anxiety, which really does have the potential to ruin your life.
Why i would be in the majority that does not progress??? Until i am 60, the chances of progression are 40%. Russian roulette!
I know that i have anxiety but i think it is the normal anxiety for these statistics. I can't live with this threat above my head. And with my triple negative status, i won't stay in the MF state for a long. So AML is really a threat for me.
Yes I should have said you'll probably be in the majority.
I honestly believe that your anxiety is greater than normal. Perhaps a chat with your haematologist would help. - if you are high risk for AML, I'm sure you would be offered an SCT, if you progress to MF. Doctors are not going to give up on us.
Aneliv9 I think your anxiety is justified. Consider how actual doctors feel when they are diagnosed with ET. Here's a veterinarian that was diagnosed and as you can see, she is very anxious, especially since she's having such a hard time getting her doctor to prescribe Interferon to slow or stop progression. imagizer.imageshack.com/img...
Full on anxiety ruins lives. I am so thankful that I didn't spend 20 years agonising over whether I would progress to MF, although my haematologist had suggested that would happen eventually.
When it happened I knew I had at least had a great life in spite of ET. Now I am having an SCT, which is massively risky, but really, how is life-wrecking anxiety ever justified? Anxiety itself is really bad for our health. If one has a true anxiety disorder, I don't believe it is ever helpful to embrace it as justified.
You’re absolutely right. I’ve been through similar, following my Dec ‘20 diagnosis, and people on this site helped hugely. The fears have subsided, if not disappeared completely. Perhaps the trick is to remind ourselves that everyone has things unspooling inside them that will eventually present as an illness. Many aren’t even aware they’re happening. Are they luckier than those of us who ARE aware a mutation or two is affecting our health? I don’t think they are. The trick must surely be to embrace the good moments and see the rest in their rightful context.
Aneliv9, please understand that I am going through this NOW. I believe my excellent consultant. I have accepted the risk, but I am focusing on life, not death.
I'm sorry I commented on your post - I meant to be helpful but obviously my comments misfired
I am not trying to dispute these figures in any way but it’s worth noting that it says this is a single centre study based on 476 patients. Some of the other experts are not so convinced by this study as Dr Silver is. Some prominent experts suggested it needs to be a bigger multi centre study. Having said that if I could tolerate Pegasys it would be my first choice because it might slow progression for a subset. I wonder if the reported shorter survival on venisections is as straight forward as it looks at first glance. As we know the majority of deaths in MPN is due to thrombosis. Hct above 45 for men is high cause of thrombosis. I know from 11 years of venisection and knowing others doing it that Hct can jump above 45 when a venisection is due. On meds Hct tends to be steady and easier to keep at a certain level. No doubt more facts on this may emerge, in the meantime best keep Hct well controlled and consider Peg or Bes if you can until better drugs come along. Of course we now also have Ruxolitinib and others in the pipeline so again these figures are historical ie going back 20 years to date.
My Dr said of that report its retrospective nature was limiting. But it does seem carefully done. I asked one of the authors how they provided for the limitations, he said they made large efforts to compensate but understood that dissent is normal. I believe this report, along with FDA approval of Bes, are some reasons for the revival of IFN.
It seems there is a pattern of risk with Plb, as you say the fluctuations are a likely factor. If there were a device like an insulin pump that drained RBCs on demand only as required that might address some of that problem.
Best near term targeted med for HCT is Rusfertide. I think the trials are going well.
I hate these statistics! There's so many variables involved with progression than just whatever treatment plan your on. I guess I'm one of the lucky ones (51%-PV) who is treated with phlebotomy and aspirin for the last 20 years and had excellent results recently from a BMB and NGS. No sign of increased fibrosis or signs of progression! Great news! More importantly I had NO driver mutations that would suggest future progression. I totally understand if your on INF and really want to believe that the drug will help you with not progressing and there's studies out there to support this MAY be possible. My MPN specialist cited in many of the studies posted on this forum is not convinced yet scientifically that INF's aid in suppressing progression. They definitely aid in preventing clots & strokes which increase survival rates. These statistics are great for the pharmacy's that are promoting their drugs!! Be careful with believing these statistics. Best wishes! Kerry
I think Drs agree that IFN is unproven on progression. The Ropeg trial had great results there vs HU (5x better) but n was very small, these really need 10+ years to know:
"The incidence of disease progression among ropeginterferon alfa-2b treated patients was 0.2%-patient years (1 case of myelofibrosis) versus 1.0%-patient years in the control treatment arm (2 cases of myelofibrosis and 2 cases of acute leukemia)."
What is becoming more accepted is IFN reducing allele, this is a consistent pattern in most IFN trials. Increasingly it looks like achieving the lowest alleles (near or below undetectable) may be particularly beneficial. Unfortunately few get to that magic level.
In the background is the long term retro study noted often here from the Cornell group. It did show a large benefit, but was not prospective.
Like I've mentioned in previous comments regarding the significance of reducing allele burden.........there are two completely opposing views among MPN specialists. For example the MD Anderson docs believe reducing the AB is important and then there are other docs such as mine (Mayo-Rochester) who have literally been involved in the AB research/also cited in many of the studies that you have posted, who are not convinced that AB is relevant at this juncture.
My last teleconference with him I specifically asked about AB. He said, "Kerry it has not been proven as of yet that lowering AB is of any significance but my mind can be changed by factual evidence. Both my MPN specialist & Hematologist do not put ANY significance on AB. My AB is at 93% which is really high!! I have very little symptom burden. For myself, I believe personally that the daily exercising /healthy eating/rest is my magic bullet for reducing any symptom burden. Works for me but it certainly may not work for someone else.
Please note as well I have no other health conditions. We are all different with how the disease affects us. I look forward to long term studies involving people who have no trace of AB and go off their INF.......how many are cured? Haven't heard of many on this forum who are cured after years of being on PEG although I do know one person who still is in remission after 10 months of being on PEG. This appears to be very rare.
It's important for everyone on this forum to keep an open mind which I certainly do. It's very very exciting to see all the new research taking place and options for treatment. We are headed in the right direction for a cure one of these years! Hope you care feeling better on Besremi and appreciate all your informative posts.
when I was diagnosed the hematologist and her team explained it like this. Your body has a secret that it can form blood clots BUT now you know this secret and we will work together to track and treat you as needed. This is the purpose of the monthly ( in my case) blood test.
These beautiful fellow MPNers calmed and educated me on my disease. Look at your food, exercise activities and lifestyle. You will live a long and happy life, there maybe more roadblocks but you deal with them when or if they come.
My daughter has been diagnosed now also. She is 21 and doing extremely well. Obviously she has questions and concerns but I do my best to keep her in her life now and not the future.
Dr Bruce Liptons book Biology of Belief is a great audiobook to listen to or ready.
Sadly I have lost friends from various cancer diagnosis over the years. Their disease journeys were fairly limited in some cases because of late stage of diagnosis and limited treatment options.
We all have a chronic disease that may or may not progress. Many individuals on here have several issues and are still living a good quality of life.
Please take time to do some Breathwork and slowdown.
No baby born EVER was given a length of time to live. I want to hug you and reassure you that everyone here knows how you feel. You are creating issues for yourself by worrying about the end of your life. Please concentrate on living your life and enjoying it. I switched doctors and got to a wonderful MPN specialist that takes care of my daughter and I.
Inflammation is the root of most issues in our body. Take the time to search this site and see how everyone is dealing with their own issues.
Thank you very much,but i really can cope with the fact that i ALREADY have more than 20 % chance of progression and in the next years this will only come up. Its just frightening. I can't live with this
My BMB showed ET but my my blood started to show PV. I had several phlebotomy and started to feel better. The hematologist said that PV could very well be the destination of my disease. I agree hopefully. Started aspirin everyday immediately after blood tests confirmed high platelets which helped with the burning feet and sore legs. I started pegasys 6 months ago. Platelets are coming down slowly, still require phlebotomy every few months. Dose 180every week with no real issues. Occasional crazy itch out of the blue but the Benadryl liquid pills seem to help with that.
I am carefully and purposely experimenting with diet, meditations and Breathwork especially at night so I get a good night sleep. I walk mostly for exercise but plan on starting some chi gong and weigh bearing exercises. I come from a large family and am the only person affected by blood issues except my daughter now. When we look back on my older bloodwork my platelets were rising after the birth of my son, 16 years ago.
I live in Canada where they do not test for or recognize allele burden as part of MPN issue. I decided my burden was rising if I switched from Et to PV in 16 years. Because I have no other health issues and still work full time we decided Pegasys was the one to try not HU. Doctor is wonderful as is her team. I will admit that I learned more from this site than the any doctor but I am okay with that and happy to have this resource.
I just get up and do my best each day. I try not to dwell on it too much. At night I am grateful to have been here another day. Baby steps. I truly believe the pegasys can be the miracle I need but I cannot just be wishful. I do my best to help my body heal and thrive each day, mentally and physically.
we are both Jak2 We switched from the first Doctor because she was not an MPN specialist. Her bedside manor was horrible and the prognosis for my daughter was very limited because her experience with MPN patients were very limited. She also could not answer some of my basic questions which were huge red flags.
I don’t deal with percentages with the new Doctor. We spoke about age of SCT and was happily told that it was made on an individual basis there was no blanket cut off at age 65 every case was based on patient need and health, not financial status. We spoke about her success in treating others and how she had younger patients and older patients than I and how different everyone was but how similar in some ways.
She wants my bloodwork each month my daughters every 6 months presently. I see her every 3 months in person but now because of the Pegasys is going so well my next appointment is in 6 months.
I understand the risk of progression and have taken the stance that I have some control by keeping inflammation down to the lowest levels and taking care of myself, so I do.
When first diagnosed I reached out on this chat and others responded. I spoken with ET patients that had it for over 30 years and really no issues once starting the aspirin.
Why would I stress out my world, my husband or children when there are some people with this disease who do not progress in 30 years. Always choose the high road for everyone involved. I did not recognize that I was feeling anxious and depressed immediately but my thought process was working overtime. A good friend is an acupuncturist and I confided in her. She helped get me out of the fight or flight craziness I was in. I see her every few months for a treatment. At that point I also found this website and devoured it. Not everyone got worse, not everyone required an SCT, not everyone ……,,,, I just turned 52 when diagnosed and found out not even that was so unique. We are a small bunch of international patients but a very wise one also. My lottery in life is not the randomness of my disease but the incredible husband, children, siblings and friends I have. My doctor is a gem. She reassured me as did this lovely community that there is hope, new drugs are in the mix that’s why it has been recognized as blood cancer.
I won’t deal in percentage because they cannot be applied across the board. We are all different ages, sexes, different driver mutations, live in different countries, have different doctors etc. Continue to stay up on everything MPN that you can control that education is positive but let go of the disease weight. You are on a long journey in your life, don’t be looking for the escape hatches instead shore up your support and move ahead. You have to find your own living support not some old chart that reduces you maybe to a colour and a corresponding out come. We are all fighters that’s how we found each other.
Thank you to everyone who helped me a few years ago when I was feeling overwhelmed. ❤️
we talked about disease progress once and we do not dwell on it. I have this part Et or PV not MF or leukaemia why would I continue to discuss something I don’t have.
You cross that bridge when you get to it. Every case is judged on a case by case basis that is good enough for me. I am not 75 and don’t need a transplant so I don’t dwell on it.
Most people will die with the MPN not from the MPN. That alone is reassuring to me.
I plan on being an very healthy at 75 year old so who knows. I am 53 now that’s so many long, happy wonderful years away.
You need to trust someone, so make that person yourself. Trust that you have a small weakness but that all your other strengths make up for that deficiency.
I could send my blood away to get a whole crap load of tests to find out a million possible scenarios for the future me but what the heck for. I know the secret my body can make blood clots, I choose to work with that info and make sure it cannot make blood clots. ❤️
I would remind you and my daughter that the world is a strange and mysterious place.
Make the best with what you have.
They are making great strides in many medical areas that are similar to our disease. The CAR T therapy is very interesting. Besremi itself is also an interesting development. Just a simple tweak to improve what’s already out there.
They reclassified us a blood cancers to create interest in developing drugs to treat us. I believe many companies have seen dollar sign ( or at least it hope ) when it comes to treating someone who will us their meds for the next 20-60 years. None of them are getting rich by us using HU, they want us on better, stronger and faster drugs that cost more. Ultimately they want more money and we will pay for it so that is the best reason to be hopeful!!
Take a look at the book Biology of Belief by Dr Bruce Lipton. Google him, he has a nice website with links to his many videos, podcast appearances and all that.
“Stress and worry will heal your disease” is not the motto for any sick person so why should it be your motto. Honestly all we can do is be proactive with our health. We know our weakness and we must adjust. There are many fine examples on this site of people living long life with a disease that was simply not very well understood. Likely we were all born with it and it arose as we aged some like you experienced the presentation of symptoms earlier and many much later in life.
Changing your mind is for the most part free. Trust that you and your Doctor working together will have a positive outcome. No one ( I hope anyway) gets a tooth pulled when they have a small cavity, they treat the cavity and makes the tooth stronger, the mouth stronger and the body stronger. Change your thought process today. You cannot cure leukaemia if you don’t have it. You are trying to get ahead of something that may never happen.
Live every single day and moment which is yours, not at progression and its end.
Life is unpredictable for normal population too.
Good luck friend for dealing this anxiety, sooner you get free its lot better to feel ! You dont need to think about this 24*7. Go for walk, exercise, read, eat lot of food ,make friends and Cheers, life is now.
I wish i could. I have serious depression from the time i realized that risk can go so up according to years of having ET. The fact that i have slightly enlarged spleen makes progression and leukemia seem inevitable to me. So for the last 2 months i cant even be functional. I cry every day almost all day.
Sorry to hear about your present condition. Enlarged spleen and all other symptoms related to MPN are manageable . I advice please dont go to to extreme thinking, and try to manage the disease and take control of yourself . Mental peace is necessary for well-being.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.