MDT and intermittent ADT offer a progression free survival advantage when compared with intermittent ADT alone.
"MDT facilitated a longer time with eugonadal testosterone as part of an intermittent hormone therapy strategy."
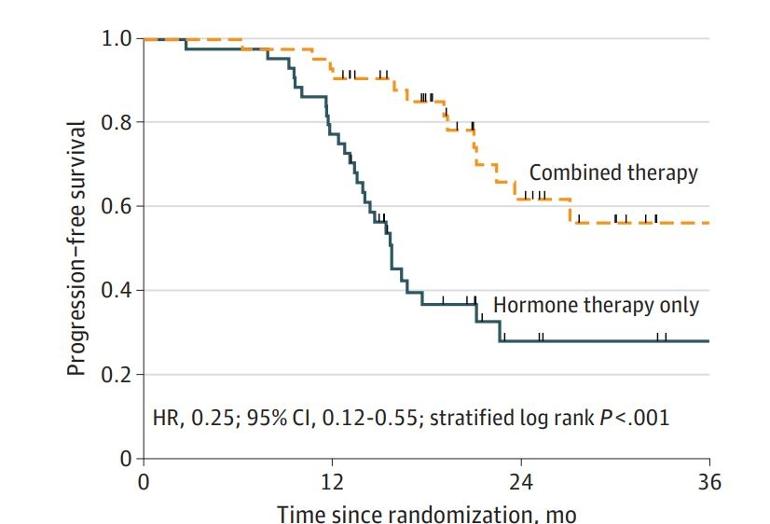
"Time to new lesion failure was longer for patients randomized to combined therapy (2-year incidence, 0.33; 95% CI, 0.18-0.55) than for those receiving hormone therapy only (2-year incidence, 0.41; 95% CI, 0.22-0.68) (HR,0.33; 95% CI, 0.11-1.0; P = .04)."
The study showed that adding metastasis-directed therapy to ADT, i.e. radiation of the prostate and the visible mets, provides a significant benefit for advanced PCa patients. You can improve ADT effectiveness by zapping visible tumor lesions.
Patients can stay with testosterone of 150 and higher for a longer time. I think this is an interesting result.
They also had around 20% less lesion progression at 2 years.
They showed the benefit of radiographic progression free survival and biochemical free survival. There is not evidence yet of an advantage in overall survival.
Sadly, that is more of the same circular logic: They treated the sources of PSA and erroneousely declared "no cancer progression" when PSA didn't increase. However, there may have been a small real effect on progression (because time to new lesions was longer for the radiation group), but we won't know for several years because the incidence numbers are very small in both groups. There will be other trials that don't make the mistake of using circular reasoning.
I thought the stampede trial had already shown the benefit of radiotherapy to the prostate for a certain population of ogliometastatic Men. When my PSMA PEt showed mets my London RO ( very SOC) ordered ‘stampede scans’ ( more basic) and deduced I would benefit from radiotherapy to the prostate However she also did SBRT to the 2 mets on my PSMA scan ( T1 and third rib) before ADT in case of a abscopal impact so she must have had evidence to do that.
My only regret is not doing more sooner ( I really wanted Lu-177 at the same time which I see is now being trialled).
No regrets re targeting my mets and prostate with radiotherapy rather than just relying on ADT, however I thought this bit of my treatment was based on evidence.
My early Lu-177 6 months later and brachy took me to a non standard radiotherapy triple, this I know!
That’s great news as that’s my current protocol. I’m waiting for TA to rain on our parade…TA is this the proof we were looking for? Or ‘no’ because longer overall survival not yet shown?
I understand that there is a value for certain people to have someone interpret complicated studies when you’re perhaps in a setting where your medical care team is not in line with cutting edge treatment.
And I also understand that the majority of leading MedOncs have significant “disclosures” with respect to funding received from drug companies. You see a 4 month benefit from OS from a new drug in the general oncology space and it’s considered “groundbreaking” front page news. RadOnc comes along saying we have this thing that seems to improve 5 year survival rates by double digit percentages (STOMP), and the harpies look for any outs to deem it unproven, tentative, temporary, or experimental.
Let’s be fair. It is problematic for drug companies to imagine people stopping their drugs for a therapy that otherwise takes an hour and is repeatable. And yes, patient selection bias is a thing - so IF you have access to cutting edge imaging in a timely manner and the money to not deal with insurance, then maybe you’re one of the lucky ones.
But I have watched this space for over 5 years and the absolute steadfast ridiculousness with which any non-chemical intervention is derided by some people is baffling. I’ve seen people go from taking positions 5 years ago like there is no “proven” value to treating the primary to there’s no “proven” value to intermittent therapy to openly mocking the leading prostate cancer urologist at Mayo. And now it’s Chad Tang from MD Anderson whose work and conclusions are being called into question. Are we serious here? I remember that Boeri study from Mayo being championed on here as some sort of vindication when it was declared that “no benefit to MDT versus ADT” in a bone-only oligomets setting, yet when you actually buy and read the thing- they hit that conclusion because their cutoff date was so short that basically a very limited number of people had died in both cohorts.
It is without dispute that cancer is a heterogenous disease- meaning every tumor has a bunch of different cell lines. ADT will kill some of them, but not all. It will buy you time, good time.
But when it comes to macro deposits of cancer, tumors, highly ablative SBrT does not discriminate or care about the tumor lines - it will, as they say in the literature, “control” that met. And now we know that there’s an immunomodulatory component to SBrT, where your cells adapt to potentially stave off new mets for a good amount of time. Oh but the “micro cancer” is still there, yes every human being has micro cancer, and it’s not micro cancer that kills you. Oh but you’re “just treating PSA”, um yes, a tumor marker that tells you how much tumor you have. And to be fair, we also know that SBrT is of far greater use when combined with systemic therapy. But maybe we should instead say, systemic therapy is of far greater use when combined with SBrT.
There are exceptions and individual examples and studies that pull in every direction. But knowing what we know now, in 2023, is very different than what we knew in 2018. Yes some people have nasty cancer that’s non responsive to treatment, and fast, yes many people have an overwhelming burden of disease that no amount of SBRT can control. And on some level you have to respect anti-SBrT people for the steadfastness with which they stick to their positions, even if the argument keeps shifting over the years ever so slightly.. “no benefit” to “it’s only a single institution study” to “patient selection bias” to “no overall survival data” to “just treating psa” to “circular reasoning” to “perhaps some marginal benefit”, in spite of the fact that nearly every major medical center in the world has adopted MDT as a vital and integral component of cancer care.
This is stressful for me but I’ll leave with two thoughts - the first is this week’s Stampede paper - comparing Enza+Abi versus Abi alone - the first group had a 30% lower overall median OS versus Abi alone - too much of a good thing with the drugs, I suppose. The second is this fun single patient study you can find on google scholar about an old guy in Italy who refused ADT and everything else because he was worried about his “performance” and only did SBRT- over and over and over again. The authors thought it was remarkable, something like 6 or 7 lines of SBrT treatment over 10+ years, still alive, Karnofsky over 90%, dude living life.
Obviously every cancer is different, and everyone responds differently to treatment. But I’ve seen very smart people bullied off these forums for thinking outside the box. And now that outside the box is becoming standard of care, maybe there’s more value in sharing stories and approaches to remarkable survival versus steering everyone back into line.
I understand Tall Allen on this point. He makes his points with scientific clarity. My oncologist suspects two spinal mets from bone scan and has ordered a nuclear scan to be certain of the situation. If oligometastatic he recommends SBRT to the sites.
By your evidence, should I argue with him to avoid this treatment if it is available and he recommends it?
There is not evidence yet that metastases direct treatment in oligometastatic PC patients prolongs life.
There is evidence that prolongs radiological an biochemical progression free survival.
Metastases are the cancer. Any direct treatment to metastases reduces the tumor load and it may delay the dissemination of the cancer.
MDT is used in many cancers and it is used in PC all over the world. I believe the only place MDT is a controversy is in this forum.
I have consulted about MDT for my oligo metastatic PC with doctors in Germany, the Sloan Kettering Cancer Center in NY, UCSF, UCLA, UCSD and City of Hope and all of them recommended I have MDT of 2 retroperitoneal nodes.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.