Role of Lu177 PSMA Therapy earlier in the course of the disease.
Sharing an Interesting Case: Response... - Advanced Prostate...
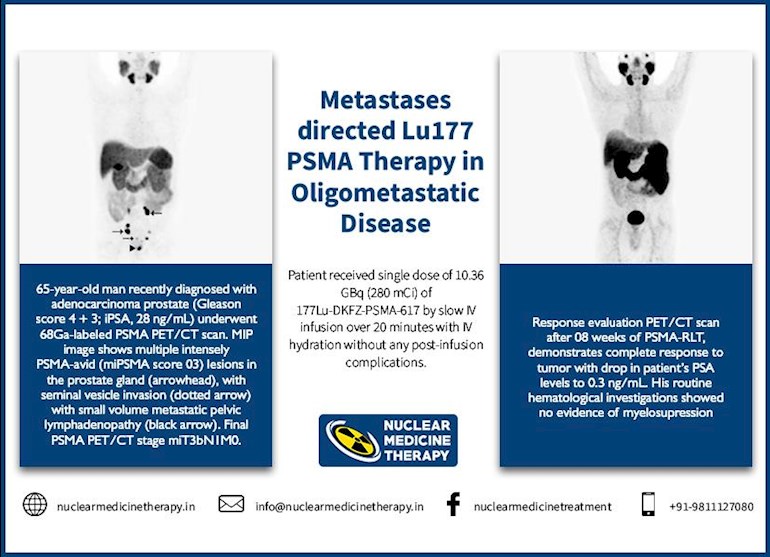
Sharing an Interesting Case: Response to Metastases Directed Lu177 PSMA Therapy in Oligometastatic Disease
Written by

ishitasen
To view profiles and participate in discussions please or .
58 Replies
•
Thank you for that. We know its not for everyone, but it appears that earlier may be better?
spencoid2• in reply to
so why is there only one trial in new York? This is fucking nuts. I don't understand the medical (highly profitable) industry. On a recent Prostate Cancer zoom meeting a brilliant doctor suggested early treatment. Is she the only one with that rare combination of intelligence and compassion?
• in reply tospencoid2
Dr. Sen been doing it early for awhile. But I guess the data is sparse
Is there any downside to earlier use of Lu177 PSMA therapy ?
Salivary gland dysfunction leading to dryness of mouth
• in reply toishitasen
seems a very small downside
ishitasen• in reply to
Well..depends...salivary gland function is important to be able to talk normally, swallow, taste food and general well being. In a patient with extensive progressive disease or with pain due to prostate cancer, the salivary gland dysfunction may be an acceptable adverse effect while a relatively asymptomatic person with small volume disease with years of survival ahead may find this adverse effect unacceptable.
Thank you for sharing. Have you seen any success with Lu-177 when the prostate has had focal ablation/ focal HIFU?
• in reply toBrysonal
That would seem to be mixing apples and oranges. LU-177 is for attacking mets, no? So what difference would it make if there was a prior ablation?
LearnAll• in reply to
You are right Anomalous. The mechanism of action of Lu177 PSMA therapy in simple words is that the radioactive isotope Lu177 attaches to PSMA..a membrane found on the surface of prostate cancer cells (PSMA avid cells). Once it attaches to PSMA avid cancer cells, it damages these cell leading to cell death (apoptosis) and thus clearing the body of prostate cancer cells wherever they are in prostate, in organs, in bones etc.Just like ADT has variable PSA response in initial months, Lu177 also has variable response in different individuals. In my case, in first 11 months of ADT, PSA dropped 99.98% (super response) In some one this can be 80%, 70% or even less. Lower the Nadir PSA, longer the survival. Longer it takes to Nadir PSA better the survival.
In the same way, after first cycle of Lu177 PSMA therapy, if PSA drops by over 50%, it indicates very good response and better long term survival. The the first cycle can set the tone for how well the patient will do with his disease long term.
The case presented by Ishita Sen above is of a lucky man who seems a super responder as his PSA dropped 98.9% just after first cycle. This indicates excellent long term survival.
Hi LearnAll - Could you elaborate on the comment “longer it takes to nadir PSA, better the survival”? Do we understand what is the mechanism involved, why would this be the case, by how much are things “better”, etc? Any journal article references would be great.
I’m trying to tease out the difference b/w this perspective on “longer time to nadir PSA” (predicting better survival) vs one that presumes the development of more castrate resistance, thus slowing the PSA drop (predicting at least a worsening disease state, and thus worse survival). I may be misunderstanding various things here.
If I should start a different thread for this, pls let me know.
Thanks!
Lokibear...I will be able to give a brief answer today as I am busy with family members due to Thanksgiving day tomorrow.Earliest study about Nadir PSA and length of survival was by Juan Morote et al in 2003. Later, Maha Hussain had a larger study about this subject confirming that Nadir PSA and Time to Nadir clearly corelate with survival. Patients on lupron who reached PSA 0.2 or less (intact prostate) and took over 11 months or more to Nadir PSA , the median survival was at least 6 1/2 years.
In 2016,, Japanese researchers led by Takeshi Sasaki explained the mechanism of Time to Nadir and longer survival. Their conclusion was "Prolonged PSA decline indicates the presence of protective fibroblasts that preserve the AR dependence of PCa cells improving length of survival." (more on this later)
Thanks! Enjoy your Thanksgiving.
Brysonal• in reply to
Reading this case the PCa in the prostate did seem to respond to Lu-177 was my reading, however my prostate has been ablated so wondering in the Lu-177 has ever been effective against PCa in an ablated prostate.
HIFU is usually used in small volume prostate confined disease. Lu177 or Ac225 psma is used in metastatic disease which expresses psma receptors. So the clinical indications are different but yes it may be effective post HIFU when patient develops metastatic disease
Thank you. The HIFU was in 2020 and failed and I am now metastatic and looking to potentially try early Lu-177 on the metastasises but not sure if it would also work on the primary which had focal HIFU
It is my experience. In 2016 , I had multiple lymph nodes metastases in the pelvis and abdomen and 1 infusion of Lu 177 PSMA made all the mets PSMA negative. PSA went down and they have remained PSMA negative until today (I had 4 PSMA PET/CTs done, last one in October 2021).
I did not have major side effects. It is not true that Lu 177 PSMA treatment causes sustained or permanent lesions of the salivary glands and dry mouth. The treatment did not affect my salivary glands at all.
Tango, I am a bit surprised that you write the Lu177 treatment converts PSMA positive mets into PSMA negative mets. I think the Lu177 treatment destroys the PSMA positive mets with radiation and the PSMA negative mets remain, should they exist.
The only thing we know is that the mets are PSMA negative after the Lu 177 PSMA treatment.. Since the PSA goes down, it is what you said, PSMA positive cancer cells were destroyed.
There could still be PSMA positive cancer cells remaining in clusters less than 4 mm beyond the resolution of the PET scanners and clusters of PSMA negative cancer cells in all the mets..
The fact that the mets are PSMA negative after the treatment does not indicate all the cancer cells in the mets were destroyed.
If the cancer is oligo metastatic and the mets are amenable to treatment with SBRT, I believe is better to get SBRT than Lu 177 PSMA. If the radiation treatment is done correctly most probable all the cancer cells will be destroyed in all the mets.
I also had two Lu177 cyles against my oligometastases. It took about 2.5 years until new mets appeared and I could treat them again with a second cycle of Lu177. I am intraductal so my cancer spreads quickly. Here is a report of my therapy:
healthunlocked.com/advanced...
Dr. Isthita Sen (image here: nuclearmedicinetherapy.in/v... ) used 10.36 GBq which is a high dose of Lu177. Usually you get 6 GBq or 7.4 GBq.
In this trial by Dr. Prive they used even lower doses with good response. clincancerres.aacrjournals.... However, the author writes he would continue with 7.4 GBq because he did not observe significant side effects. I got 8 GBq with my last cycle because my doctor said he did not observe any side effects even with 15 GBq.
It seems that the patient presented by Dr. Sen did not get his prostate ablated before the Lu177 therapy. I would recommend a prostate ablation and then a Lu177 therapy against the mets because I know a case where the Lu177 therapy could not remove the cancer in the prostate completely, just partially.
Dry mouth is a bad side effect. You need your saliva to keep your teeth healthy etc. With Lu177 the saliva is sometimes reduced but that goes away after two to three weeks. As you can see from the image presented by Dr. Sen, the patient still has fully functional salivary glands.
Its different with Ac225 though. Two cycles can destroy your salivary glands. Below is an example, apparently by Dr. Sathekge in Pretoria, who treated the patient with Ac225.
This patient had very advanced PCa so he had to sacrifice his salivary glands as you can see in the last image. However, he got rid of the very advanced tumor as well.
Advanced PCa patient getting Ac225 after Lu177 therapy
So it ONLY works when you are hormone sensitive- doesn’t prostate cancer evolve to not express PSA ? So the sooner in your journey the better? Would it come to a SOC where a man would get off all medication and then use Lu 177 to erase any cancer that pops up? I maybe simplifying - if you were newly diagnosed with little spread this could cure you?
ishitasen• in reply to
No in fact PSMA therapy works better when disease is castrate resistant. PSMA is an enzyme which drives the growth of a cancer cell and is upregulated when the cells become castrate resistant. PSMA therapy is almost always used in castrate resistant state. However some recent data demonstrates that lu177 psma may also be used in hormone sensitive patients with small volume disease with good results. This was one such patient who was hormone naieve but could not take hormonal therapy due to another medical condition. He did exeptionally well, achieving complete biochemical response and near complete radiological response with just one dose of lu177 psma. We went on to give him two doses more and he remains in complete PSA response 2 years down the line.
• in reply toishitasen
Thank you for your thoughtful and educational response. My husband was oligometastatic and received SBRT to his 3 small bone Mets along side erleada and of course lupron < .02 PSA going on 2 years. I am the one that educates us so he can focus on his health.
There is a clinical trial at the MSKCC trying to prove that Lu 177 PSMA is effective in hormone sensitive cancers.
Anecdotally , for my experience and GP24's experience and by conversations with the doctors at the TUM in Munich (they showed a bunch of hormone sensitive patients treated with Lu 177 PSMA), Lu 177 PSMA is very effective in hormone sensitive cancer.
I hope the MSKCC trial will prove it and the SOC change and use this systemic therapy with no major side effects unless there are extensive bone mets.
The questionable results of the Vision trial (only 4 months median life prolongation and a lot of negative side effects) happened because of the population they treated. They were patients at the end of the road after many therapies ( anti androgens and one or more chemo treatments) and I believe some of them with many bone metastases. It is remarkable that in those patients Lu 177 PSMA could help to prolong life.
It does not cure metastatic PC by it helps to gain some time before reaching the end.
What is the clinical trial number at mskcc and who is the leading MO?
I believe is Michael Morris
spencoid2• in reply to
i think it could but the money hungry medical industry does not give a shit about us, they just want their $$$$$$$
I had 2 sessions of LU-177 & PSA went from 18 to 2 in a matter of months but months later was back to 19. I will never know why they stopped the treatments at a PSA level of 2.I was told to go back to the ADT & then chemo before asking for LU-177 again.
Now Firmagon has my PSA down to 0.8 so hoping to keep it there.
Life is not good & QOL is 0 but im alive & thats a big +
Thanks for posting this case and the two year follow up. I would have been inclined to follow it with full prostate and pelvic LN fields RT for co presence of PSMA negative population. But cannot argue with such success.
I would love to give LU177 treatment a try since all of my mets seem to be in lymph nodes at this point. Just not sure I want to pony up the $60k plus it can cost to go overseas for treatment. Not sure why the USA only allows treatment in "trials" while much of the rest of the world has been using it for years. There is a lot about the American medical institution that thoroughly pisses me off.
Hi Joe, I've had three LU-177 treatments this year at Fortis Medical Research Institute in New Delhi with Dr. Ishita Sen. The LU177 infusion cost around $6K per infusion, roughly half the cost of treatment in Germany & Europe. This is the same medication they use in Europe and it is flown in from Germany. You can fly to India for around $1K, stay at a hotel for a week (around $700 or less). So treatment can be possible without spending $60K. If you have any questions on getting there, feel free to PM me.
Thanks for the info! How many treatments are typically recommended? I have heard varying numbers. Also, how is the LU177 working for you?
It varies on a patient's medical condition and how well they respond to this type of treatment. A PSMA Pet scan would be necessary to see if a patient is a good candidate for this type of treatment. At Fortis, these scans cost around $350. In the United States, they run anywhere from $2,000 to $5,000.
The one I had done at the university of Iowa was $2200
Was Iowa a clinical trial? Other members previously said UCLA or UCSF were now charging $21,000 since FDA approved. So I did pay $2,600 -$2,700 back in clinical trial days at UCLA.
Greghouston is the $2-5 you wrote 2,000 -5,000 or 25,000?Are those clinical trials or FDA approved treatments.
UCLA / UCSF were reported to be charging $21,000 after FDA approval. Around $2,600 in clinical trials before FDA approval.
My apology, I meant anywhere from $2000 to $5000. I think I read that they cost around $2000 at UCLA. The prices will come down after they become more available around the country.
Greghouston. Pet scans for prostate cancer are expensive in the US. A Choline scan costs $16,000+ at Mayo, Axumin scans have some wiggle room but are close to that. PSMA scans that are FDA approved just this past year are reported to cost $21,000 at UCLA and UCSF. Several years ago I would have had to pay $10,000 for a clinical trial scan at MSK in NYC. But went to UCLA for a clinical scan trial at $2,600. So it doesn't seem possible that a PSMA scan that isn't in a trial costs what your indicating. Please post evidence of such low costs.
Of course in Australia they reportedly cost $800.00 US dollars.
My first PSMA scan done at UCLA last year was billed at $22,000 with a co-pay of $3,300 using Medicare and Blue Cross supplemental. My second scan a month ago was now covered 100% by Medicare. Hallelujah!
In Australia a PSMA PET CT is free with Medicare at a public hospital. Costs about A$800 at a private hospital.
Do you know how well Lu-177 works for BRAC2 CRPC? I was recently refused a Lu-177 clinical trial because I am BRAC2. The sponsor didn't think it would work well for me even though my Onco disagreed.
Response to PSMA targeted radioligand therapy is possibly multifactorial, being related to the heterogeneity of PSMA expression, In a study published in European Eurology in 2019, the researchers have provided robust evidence that PSMA receptor expression is associated with BRCA 2 loss and deleterious DNA repair aberrations. Intuitively then patients with tumours harbouring these defective genes should show a better response to PSMA based radioligand therapy than those who don’t. Interestingly the same was not proven in a small retrospective study published by the Heidelberg group where pathogenic DDR aberrations were not associated with exceptional responsiveness to PSMA-RLT. While larger studies are required to prove or disprove the association of the defective gene aberrations with response to PSMA therapy, most of the patients with BRCA 1 or 2 mutation in my practice have done better with lu177 psma therapy than those not harboring the gene.
Do you have any views on the use of Veyonda with Lu 177? Or radiosensitizers in general? Thank you, Nicola.
NickI remember reading that combination used in Australia early 2001 maybe late 2000. Those reports stated three times the effectiveness over straight LU-177. Anyone from Australia have any update on LU-177 and Veyonda?
It is said that the combination of Veyonda with Lu 177 is highly beneficial. You can Google recent info about it. Noxopharm is the company and its CEO Graham Kelly apparently cured himself of APC with Veyonda. It’s not generally available yet but Noxopharm has entered into an agreement with Genesis Care here in OZ to provide it together with Lu 177 on compassionate grounds. Lu 177 is about A $10 000 / treatment. Don’t know what the cost of the Veyonda is.
Veyonda sounds very interesting in conjunction with Lu-177. It looks like Darrt2 clinical trial in the US will be using the combination and the patent is agreed in Europe. Dr Sen as you are an expert in Lu-17) will you be asking if you can add it on compassionate grounds like Genesis?
I'd like to second the suggestion that Dr Sen look into adding Veyonda to her treatments. I suspect I will be needed to travel to her hospital in the future for LU-177 and would like to have the best response possible. Hopefully she could provide both treatments together to patients in the hormonal sensitive state.
Thank you so much for sharing this Dr Sen
Is the available in Canada?
Not what you're looking for?
You may also like...
Oligometastatic prostate cancer: Metastases-directed therapy?
New paper below.
As someone who received treatment for a single spiny met at L5 last year, I am...
PSMA LU177 THERAPY IN GERMANY
Hi All. My dad has mCRPC since June 2015. Tried Docetaxel, Zytiga, Xtandi, Radium . Nothing helped...
Addition of Metastasis-Directed Therapy to Intermittent Hormone Therapy for Oligometastatic PC. The EXTEND Phase 2 Randomized Clinical Trial
MDT and intermittent ADT offer a progression free survival advantage when compared with...
Excellent response to Ac-225-PSMA-617 in South Africa (update)
I updated the South African trial info based on new info on 73 treated patients. In 79% of...
Why the need for an FDG scan in addition to a PSMA scan?
I have had three negative PSMA scans at UCLA in the last year. A number of those more knowledgeable...
Related Posts
 Exceptional Response to Pembrolizumab in a Patient With Castration-Resistant Prostate Cancer With Pancytopenia From Myelophthisis: A Case Re
Exceptional Response to Pembrolizumab in a Patient With Castration-Resistant Prostate Cancer With Pancytopenia From Myelophthisis: A Case Re Adding carboplatin to chemotherapy for mCRPC in post-second generation hormone therapy setting: Impact on response and survival
Adding carboplatin to chemotherapy for mCRPC in post-second generation hormone therapy setting: Impact on response and survival  Need an Advise and Info on Very Experienced Doctors and Centers to do Proton Treatment of the Prostate in Oligometastatic Setting
Need an Advise and Info on Very Experienced Doctors and Centers to do Proton Treatment of the Prostate in Oligometastatic Setting According to PSMA PET Scan all metastases found are in bones; so after discussion with Oncologist about options, Xofigo (Radium-223) is next
According to PSMA PET Scan all metastases found are in bones; so after discussion with Oncologist about options, Xofigo (Radium-223) is next Some Things To Ponder As We Age
Some Things To Ponder As We Age