Dr Abe Morgentaler interviewed on Grand Rounds on 'Saturation Theory' and testosterone treatment for men with and without prostate cancer. His conclusions are that testosterone above a level of 240-250 ng/ml dont affect progression, or initiation of prostate cancer. If true this makes the need to take TET to zero during ADT treatment not only needless, but harmful for men. Its a bold premise that goes back to Dr Huggin's original 1941 study on which most SOC for TET supplementation is based. The original study concludes with the statement that, "Testosterone activates prostate cancer." This conclusion was based on (wait for it) one man given TET supplements for 2 weeks...I am not kidding. So I underwent 21 months of ADT with TET below 10 ng/dl for what reason exactly? And now I may be at risk that it never comes back? There are many things in the current SOC that are treatment 'over kill,' low TET being one of supreme importance to men and QOL. The high points of the interview, its LINK and Dr Morgentaler's medical paper used in the interview are included.
Min 4:18; testosterone is a brain hormone.
Min 7:00; testosterone does not cause, propagate, or worsen prostate cancer.
Min 11:05; belief that testosterone is dangerous in prostate cancer Patients is not founded on any research.
Min 13:25; Dr Huggins, 1941 publication is the current basis for SOC. States; “Testosterone activates prostate cancer.” Conclusion was founded on three patients given testosterone for two weeks after which only 1 man’s results were published.
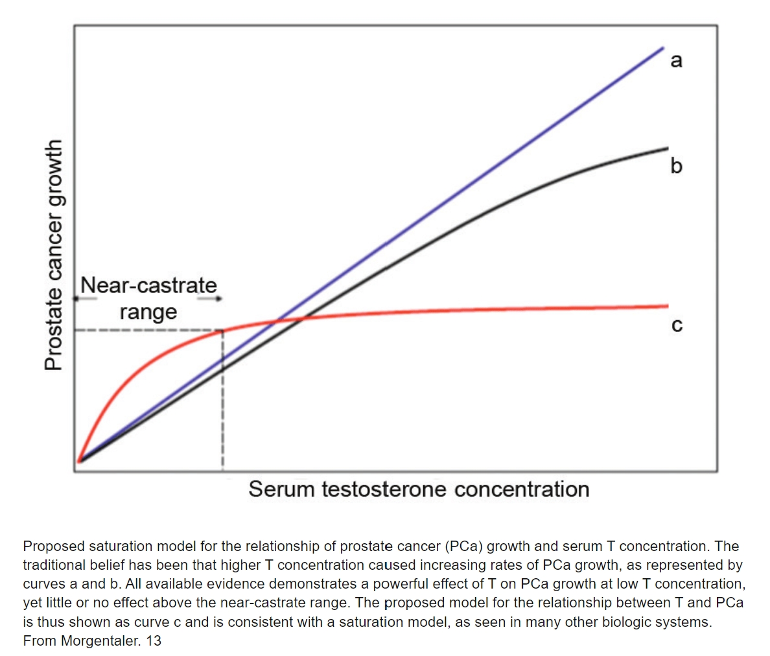
Min 14:52; Saturation Theory. BPH, PSA and tumor volume are not correlated with testosterone levels. A paradox exists. Lowering testosterone always lowers PSA, but increasing testosterone does not increase PSA; it rises but then levels off.
Min 16:35; prostate cancer needs testosterone, but the saturation point above which these cells cannot use more testosterone is reached at a low level, 240–250 ng/dL.
Min 18:35; men with prostate cancer, who receive testosterone are at no greater risk of progression than those that do not receive it.
Min 20:10; testosterone deficiency is associated with significant health issues that affect men. Diabetes, osteoporosis, dementia, metabolic blood effects, sexual function, and others.
Min 21:20; Australian study of 1000 men treated with and without testosterone. After two years, the incidence of diabetes was 50% less in those treated with testosterone. Some that started with diabetes that were treated with testosterone were cured.
