These are questions that get asked, or referred to, every day, on here. So, as none of us are doctors, I thought that 'hearing' the replies from the horse's mouth, so to speak, might help people understand. ")
Top 10 Myths of Thyroid Disease: These are... - Thyroid UK
Top 10 Myths of Thyroid Disease
Written by

greygoose
To view profiles and participate in discussions please or .
47 Replies
•
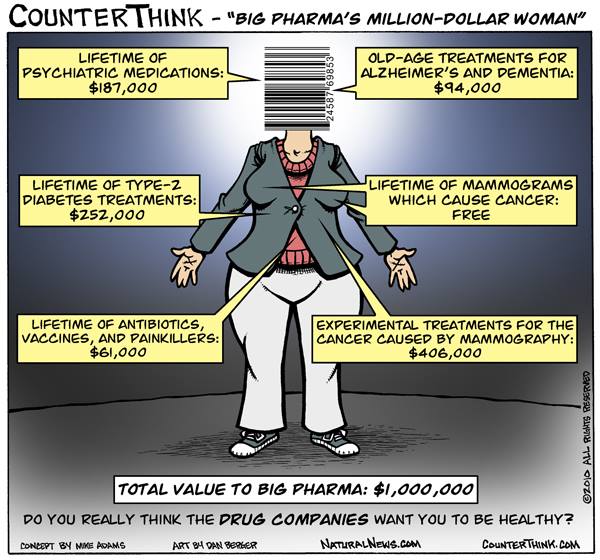
Why cure disease when they can make so much money from it?
I wish the same amount of advertising would go in to promoting healthy lifestyles as telling us we can pay them to beat cancer, etc. I don't believe there's a lot of research that's altruistic in nature, & I've a friend who works for a clinical trials charity. >
They'd go bankrupt if someone actually found a cure for cancer. In fact, there's a rumour that a cure has already been found, but Big Pharma have suppressed it!
There are different types of cancer for every type of cell in our body, so a generic cure would be a clever thing. I imagine they'd supress a cure for any, though the difference in treatment for the have's in society is considerably different.
Never mind a cure, it would be more to the point if they started looking for the cause ... but there's no money in that so that's never going to happen.
I heard that greygoose about 10 years ago. The lady who told me said not to give any items to cancer charity shops and not to donate money
Yes, I heard that, too. You don't know what to believe, do you.
Perhaps a little off-topic, but slightly related... I refuse to give a single penny to Cancer Research UK as their policy on childhood cancer stinks to high heaven! Less than 6% of their income is divided up between around 200 different varieties of childhood cancer whilst a whopping 43% is spent on lung cancer of all things! Childhood cancer research gets around 0.9 of a penny from every £1 raised and, of course, all the execs get massive 6-figure salaries before anyone else gets anything! In the meantime, families are having to raise huge amounts of money just to be able to send these kiddies to America in the hope of accessing a life-saving vaccine against Neuroblastoma there... Many do not make it, but hey, CRUK continues to rake it in... Their annual financial breakdowns make for infuriating reading...
I think most of the money goes on advertising and board-level salaries.
I thought it went straight to Big Pharma.
Nah, the directors of many charities are stunningly well paid.
What, you mean there's nothing left for Big Pharma??!!
I did a stint in my local charity shop as a volunteer, the charity which helps children in Africa. I walked out after 2.5 months as I was so disgusted at its head office policies.
When I worked in publicly funded clinical trials the private ones were really seen as the dark arts. No accountability, nothing known about any of the methods or anything that was planned. Specifically I was looking at recruitment of patients, and the kind of reasons patients don't agree to take part or drop out. This is a constant problem in clinical trials, and some trials are non-viable because they are so unappealing to patients. For example I was aware of one altering how insulin was deliver to children with diabetes. Even tho the system they wanted to test was less painful and invasive than what they already had, they had all had a painful process to get into the routines they were already using, and no one wanted to mess with theory kids routines. But no one knows how the private companies recruit to trials like this!
But a thing that shocked me overall as a sociologist/social psychologist, is that the ppl who research how clinical trials get done completely swallow and accept the medical view of things. Whereas sociologists in other areas are extremely critical, or at least distant, from the way the research subjects see what they do - for example physicists can be very angry about how they're analysed by sociologists, because it downplays what they think is the important bit, the actual physics stuff. But sociologists who are almost embedded in clinical trials also get amazing access to everything, which is a constant problem in sociology.
Oops, very long off topic post ")
My friend left Big Pharma, & has worked for charities, the NHS, & back to charity work. We've had chats about the ethics on several occasions, though it still makes me queasy thinking about the hope & desperation of people with terminal illness' who get the placebo. Even after all the testing that's done on critters. the failure of meds that get into our system because the results are stifled.
I think place is are quite rarely used in clinical trials. The ethics the leader of my unit believed, was that patients should only be put into a clinical trial of nobody knows which treatment arm is better for them. The majority of the time this is taking something called 'standard treatment' - what they'd be given anyway, and comparing it with the new treatment. Which is often a higher or lower dose of the standard medication, or a slightly different mix of drugs, etc. The argument is that if there's any reason to believe they'd be better off on one of the two treatments, they should be given that.
But an alarming thing about clinical trials is they are big Heath Robinson type rickety structures. This woman was a statistician that worked on methods for designing trials - she didn't do more than consult on actual designs. But the individual doctor or research nurse that is administering the trial to patients will have had only a half day of training, won't have met anyone on the trial team, and will be running dozens of trials, at the same time as trying to run their ward or clinic and do their actual job - working on the trial is extra stuff they probably aren't even being paid to do! That's what amazes me, that usually someone from the trial team can't even go down to that site to do spot checks. Because there are hundreds of hospital departments doing it, but an office of maybe 20 people working full time, also running loads of trials! It's crazy.
One of the big ethical issues I think is that people want to go on trials because they'll receive better monitoring and care not available on the NHS. This is considered very ethically wrong by the professionals, to the extent they almost deny it happens.
I was talking to a friend recently who is on a clinical trial. She mentioned that she was made to lie down for ten minutes before her blood pressure was taken! Really struck me because this is the definition of how blood pressure should be taken. But of course we know it never happens in the GP setting!
How many know that when taking BP you should lie down. I had never heard of that before and always in the surgery you usually sit.
And they normally hustle the arm band on you the minute you arrive, all hot and sweaty because you had to run so as not to be late!
Oh, I'm not sure about actually lying down, but you are supposed to rest for ten minutes before it's taken.
Obviously a very different reading than if you've just been walking around.
I was taking part in a pre diabetes study and I was tested and measured for all sorts of things. The thing that surprised me most when I got the results of all the tests was that my blood pressure was amazing. It was explained t me that the nurse was g8ng to take three read8ngs at five minute 8ntervals. I was not to talk to her while it was happening as that can mess with the read8ngs.
I sat in a big comfy chair and when the the came it all happened as she said it would. When I saw the results I was amazed. I know I’m tak8ng pills fir high blood pressure but even then I’ve never had it so low, so yes I agree you get better care if you are on a medical study. I know how to take my blood pressure now and when I take my readings at home I do it them same way and my surgery are quite happy for me to bring my results in.
But disappointingly within clinical trials ethics it is denied that people get better treatment when they're on a trial. It's considered a bad reason for agreeing to take part!
For me the really disappointing bit was being part of the control group which meant I had nothing other than a leaflet telling me how to reduce my blood sugar - diet and exercise. There were two other groups that got two different amounts of help. On the other hand had I not been on it I wouldn’t have been tested when I was and found to have T2. As it was I discovered low carb, high fat and diet doctor etc. So it was worth it for that. You on.y get the care because they want details for their study, they measured every part of my body. It was weird. I mean what does the length of your lower or upper arm or leg have to do with T2. Maybe a lot, who knows!
They probably don't know themselves if it has anything to do with it, but want to find out. And they'll only find out by measuring everybody.
I once volunteered for a clinical trial. I found it fascinating and asked many many questions which irritated the doctor doing the tests - they threw me out!
Hehe!
• in reply toBadHare
I had breast cancer The only that saved me was total mastectomy
It's all a bit scary, & a terrible pressure to put on hospital staff & patients if it's not constructed & monitored properly. I'm sure you're right about patient monitoring, though wrong when the additional care could be the contributing factor rather than the treatment itself.
I had no idea BP was supposed to be taken that way. Mine's always low, aside from endo appointments as they make me so stressed!
I might have miss-spken to say specifically lying down. But you are supposed to rest for ten minutes.
I heard on the news this morning that they are very close to a blood test that can be used to detect cancer. I hope it's true. x
Thanks for posting - I think we've guessed this already. Just think how much the NHS would save if the doctors learned what causes symptoms - and how to relate symptoms to the patients' problems.
Myth: My doctor says I don’t have Hashimoto’s because of my blood tests.
Kernel of Truth: Thyroid antibody tests are positive in many people who have Hashimoto’s.
Fact: Over 40% Hashimoto’s may never have positive antibody tests. Negative antibody tests do NOT rule out Hashimoto’s. In many cases it only shows up on the ultrasound.
Does anyone know how hashimoto's would show up on an ultrasound?
Well, it would only show up once some damage is done. But they can tell if the damage is typical of Hashi's or not.
Thanks. Looks like I don't have hashimoto's in that case. I'm just intrigued (as I'm naturally curious lol) as to how that damage would show up. Nodules? Change in size?
You don't have to have Hashi's to have nodules. Most people have them. But, change in size, yes, definitely. Also the texture changes.
memorangapp.com/flashcards/...
Only click on that link if you're not squeamish! But, if you scroll down, you will see lots of photos of thyroid glands, in different conditions, and one of a Hashi's thyroid.
OMG that's fascinating! Thanks for the link! The SIZE of that goitre! And somehow I never imagined a thyroid looking like a symmetrical piece of steak! 
I tend to gain weight easily and I saw you post something someplace about eating more to lose weight. I am USA so my labs are also : vitamin D 25 hydroxy D3 is 35 ng; vitamin D 25 hydroxy D2 <4; 25 hydroxy vitamin D 35 ng; B-12 is 588 PG/ML standard is 200-910; TSH 2.01MCIU/ML standard 35-4.00 MCIU/ML; T4 1.1 NG/DL standard IS.8-1.5 NG; T3 135 NG/DL standard is 58-159 ng
My blood counts seem okay to me but from what I understand you saying, a person needs to eat 2500 calories a day. I am only eating 1200 to 1500 calories a day. MY Dr. gave me 125 mcg of levothyroxine and I asked to reduce it to 112 mcg because the 125 mcg seems to cause me heart palpitations. . Of course I think being more sedentary and older aged has a bit to do with it. MY husband puts weight on easily too and he has no thyroid issues at all.
Regardless, I have been on health unlocked for years and I have read a lot on here. I thought I would ask you what you think before I go to my doctors office appointment.
Thank you ahead of time for your assistance.
Well, first of all, you need the right tests. You need FT4 and FT3. I'm not sure about your T4, but your T3 is definitely not an FT3, so tells us nothing.
However, your TSH says that you are under-medicated, and you won't lose weight if you're under-medicated.
The reason you need the FT4 and the FT3, apart from just knowing their levels, is that you need to see how well you convert T4 into T3. It's low T3 that causes symptoms like weight-gain, and difficulty losing it.
There can be many reasons for poor conversion, but one of them is not consuming enough calories. You need calories to convert. So, if you have a conversion problem, and if that problem is caused by low calories, then yes, you need to eat more.
Not what you're looking for?
You may also like...
Myths and fallacies in thyroid disease
@[40134] will appreciate the goitrogens bit!
It is pretty sad that basic information needs to be...
Treatment of thyroid disease
Reading various posts makes one wonder why thyroid disorders are so poorly understood and treated....
Thyroid Eye Disease
I am so angry and upset with this disease. I just wish that it would go away. People on the outside...
Thyroid eye disease??
I was wondering what I should look out for in regard to TED? Apart from the symptoms listed on...
Just don’t do it: 10 exercise myths
An awful lot of members feel that they must fall in with numerous edicts regarding exercise.
I...