I was just diagnosed last week. Here is the layout of the biopsy results. 13 cores with a combination of 3+3=6 and 3+4=7. I meet with the doctor on Monday, He has already ordered a PRolaris Genomic test. Should get that back in 4 weeks. I am going to look at all options before making any decisions. I am 58 and healthy. Question: Has anyone with similar biopsy results had focal therapy?
Thanks,
Marc
Final Diagnosis
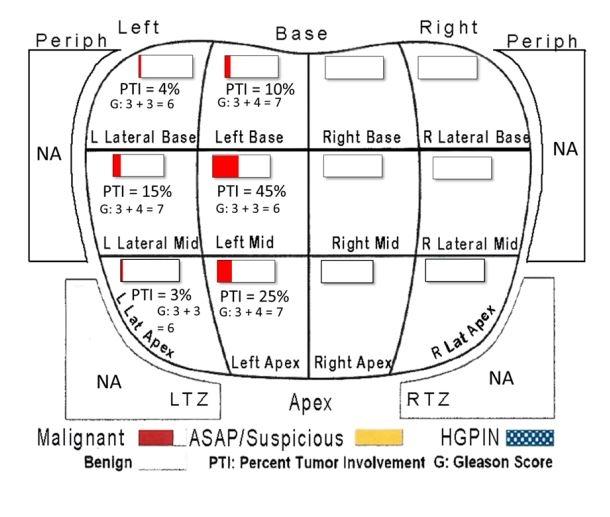
A. Prostate, left lateral base, biopsy: Adenocarcinoma of prostate, Gleason score 3 + 3 = 6, Grade Group 1, involving one core (0.5 mm, <5% of tissue present)
B. Prostate, left lateral mid, biopsy: Adenocarcinoma of prostate, Gleason Score 3 + 4 = 7 (pattern 4 = 5%), Grade Group 2, involving one core (2 mm, 15% of tissue present)
C. Prostate, left lateral apex, biopsy: Adenocarcinoma of prostate, Gleason score 3 + 3 = 6, Grade Group 1, involving one core (<0.5 mm, <5% of tissue present)
D. Prostate, left base, biopsy: Adenocarcinoma of prostate, Gleason Score 3 + 4 = 7 (pattern 4 = 5%), Grade Group 2, discontinuously involving, one core (1.5 mm, 10% of tissue present)
E. Prostate, left mid, biopsy: Adenocarcinoma of prostate, Gleason score 3 + 3 = 6, Grade Group 1, involving one core (7 mm, 45% of tissue present) Perineural invasion present
F. Prostate, left apex, biopsy: Adenocarcinoma of prostate, Gleason Score 3 + 4 = 7 (pattern 4 = 10%), Grade Group 2, involving one core (2.5mm, 25% of tissue present) Perineural invasion present
G. Prostate, right base, biopsy: Benign prostate tissue
H. Prostate, right mid, biopsy: Benign prostate tissue
I. Prostate, right apex, biopsy: Benign prostate tissue
J. Prostate, right lateral base, biopsy: Benign prostate tissue
K. Prostate, right lateral mid, biopsy: High grade prostatic intraepithelial neoplasia (HGPIN)
L. Prostate, right lateral apex, biopsy: Benign prostate tissue
M. Prostate, PI-RADS 4 left apex PZ, MRI-guided biopsy:
Adenocarcinoma of prostate, Gleason Score 3 + 4 = 7 (pattern 4 = 10%), Grade Group 2, involving four cores (19mm, 35% of tissue present) Perineural invasion present
