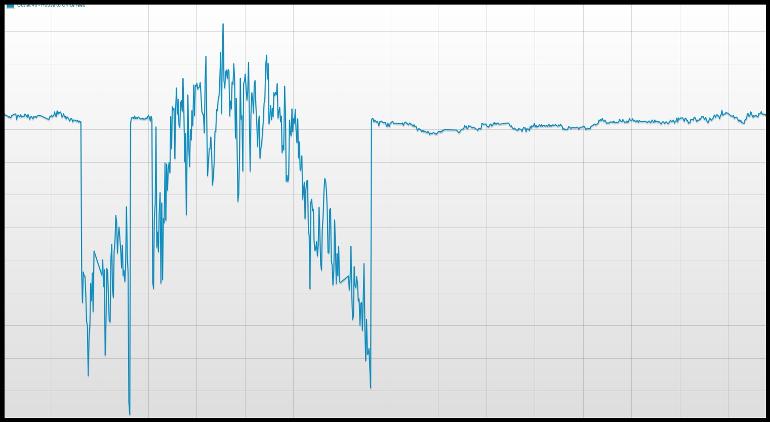
At first, it will sound as irrelevant to PCa, but my belief is that the medical community should learn from other industries when prescribing dosages. In a nut shell, more can be disastrous. Today, Sunday morning at 10 AM, as you can see from the attached graph, the grid voltage went crazy. Grid voltage (nominal value: 230V +10%/-15%) went as down as to 136V on the graphed phase, causing a led lamp to dim-off completely, and up to ~270V on the other 2 phases of the 3 phase low tension distribution system. You may want to how/why this happened. The answer is easy: Sunday morning the grid power consumption was at its lows, the sky was clear and there was also a light breeze of air. The photovoltaic and wind production plants were pumping energy on the grid at their fullest, while the overall consumption was low. The perfect scenario for a black out! If you look at the graph closer, you will spot out that stability returned twice after deep notches. Grid protection was probably auto-activated to shed off photovoltaic and/or wind power plants, or compensate for the unused real/imaginary power in any other way.
Now you may understand my Bicalutamide maneuvers. More, than needed, Bicalutamide may promote castrate resistance . Well, this is relevant to PCa. No?

")