So my question is, if for example, you have a 2% risk of having a stroke in any one year, over 5 years does that mean you have a cumulative risk of 10% or does the risk remain at 2%. Someone kindly posted this informative video but I wasn’t sure whether what he was saying about risk was correct. I think he actually said that the risk over 5 years of having a stroke with score of 2 was 1 in 5 which I don’t think can be right, otherwise anticoagulation would be recommended earlier?
Stroke risk for statisticians - Atrial Fibrillati...
Stroke risk for statisticians
Written by

Sixtyslidogirl
To view profiles and participate in discussions please or .
Read more about...
28 Replies
•
BobDVolunteer
Yes the risk is accumulative so after five years is 10%. This is what I have always been told since stroke risk was first mentioned to me in 2007. Dont forget CHADS2VASC2 then comes into play to further "tune" the risk calculation.
Thanks. That’s what I found difficult to get my head round.
Blimey I hadn’t realised this or thought of it in that way - I’m assuming the risk is due to episodes of AF since this is when blood pools - kind of makes sense actually that the chances of it happening is greater over a longer period of time - Does the risk decrease based on the number of episodes of AF in that case (which logically makes sense to my brain)?
At the moment my episodes are every 2-3 days lasting between 2 and 8 hours - Ablation date finally through and due in a week …thank god!! Fingers crossed it works/resolves/improves 🙏
I think it also depends on your family history too. In my case I’m the 5th in line on my father’s side to have had heart disease. My father died of Coronry Thrombosis as did his father. My father’s grandfather father died of Heart Failure. and his father died of Heart Disease. I was born with congenital heart disease as was my sister. My mother had a Stroke,
I dread to know what my percentage would be.
I watched the video. The risk which he stated was 2% for a year 10% over 5 years and 20% over 10 years. (1 in 5). Intuitively I suspect that the risk of stroke against time is not as linear as this statistic suggests. I assume that the risk of stroke increases with age. The concept of af burden may be informative in this matter. I recently read an article which suggested that risk for a cardiovascular event increases by 30% with each doubling of individual af burden.
If true I would presume that this aspect of risk will plateau once an individual is in permanent af. I think that the development of further comorbidities as we age is likely to increase af burden and/or risk of a cardiovascular event.
I’m still not sure you can add up probability like that. I’m going to check with a statistician and report back. If your score is still the same, then your risk will be the same. Just because you didn’t have a stroke in year 1, does not mean I don’t think, that you are increased risk in year 2. Just like if you toss a coin, it doesn’t matter how many times you toss it, previous outcomes do not affect the 50/50 chance of getting heads or tails.
• in reply toSixtyslidogirl
I'd be very interested in hearing what you find out. I'm not a statistician but it sounds off to me. Certainly risk of stroke increases with age but I really don't understand how the supposed 'accumulative risk' works.
I also think that when dealing with huge numbers of people as, for example, the NHS is, statistics can be useful to set up models for treatment, but on an individual level they are not far off useless. (imo) Also, as we know, statisics can be used to prove almost anything when applied in ways that they're not designed for.
I think if you look at it as a 98% chance of not getting a stroke each year (although I suspect this decreases with time), and therefore do ,98 to power of 10 (.98 x .98 10 times), you get an 81.7% chance of not getting a stroke in any of 10 consecutive years. So that’s an 18.3% chance you will have one or more strokes in the 10 years. Not exactly 20% but near enough to be a concern.
You're right, I'm not a statistician but I did study them and used them a lot in my career.
Statistics has no knowledge of prior events so, the fact that you don't have a stroke in a given year has no effect on your chances of having one the next year. All other things being equal of course.
If risks were cumulative and you had a 1% chance of winning the lottery, if you lived to be a hundred you'd be guaranteed a win!
I can’t claim to understand it but my statistician friend tells me that the risk is indeed cumulative, but still only a risk, not a certainty. Unlike a coin, we carry the risk with us from year to year. My brain is hurting have to say.
Hi,
I think the best way to think about this topic is, if we assume the risk is a straight 2% per annum, is the greater length of time you are exposed to that risk. So the risk at the end of the first year is 2% (ie 2 in every hundred people will have a stroke) then after a second year the risk would be 4% (ie 4 people in that hundred will have had a stroke) and so on as each year passes.
I agree statistics and probabilities are very confusing. Two things to always keep in mind, firstly recognise the difference between relative risk (i.e an increase of 5% in a factor) and absolute risk (ie the real risk factor). Secondly, be aware that probabilities are based on large datasets, they do not forecast what will happen to any one individual in that data set
Good Luck
it’s interesting as my cardiologist looks at Chad score then looks at each of his patients individually and advises to go on Anticoagulants or not. In my case if I go into AF I’m immediately on Apixaban for a month and provided I’ve been in NSR for that time he switches me to Aspirin. I’ve just turned 66 and he said when I turn 75 then full time Apixaban. Now I guess if my AF frequency increases then he will reassess, I had AF twice last year and once this September.
I think you will find you do add the risk for each year ie if the annual risk is 2% after 10 years there is a I in 5 chance of a stroke. Of course that is only true if the 2% is a reliable stat based on a big enough sample and you are Ms Average.
Also worth noting is that Prof Richard Schilling does not link AF directly with increased stroke risk (see his YouTube channel). Once in you 70's+ the risk of stroke rises for more general reasons - I heard some good advice on here a while back for avoiding strokes when getting up in the morning, which if memory serves was as follows:
Wake up wait 30 secs, sit up in bed wait 30 secs, swing legs out of bed wait 30 secs before standing up.
Statistics are baffling to most of us if we aren't statisticians. What the heck does having a 43% lower risk of having a stroke or pulmonary clotting event when taking Apixaban/Eliquis actually MEAN, and what is the percentage risk of NOT taking it? Without knowing the risk levels precisely for AF compared to not having AF and the actually quantification of the reduction in risk levels by taking a particular pharmaceutical, we can never make our own intelligent decisions.
If I have a 1% risk of being killed in a road traffic accident, and driving in a particular way reduces that by 73%, what does that make my specific risk, for example?
This quotation from the originator of CHA2DS2VASc is especially interesting, I think: "A CHADS2 of 0 is not low risk, and stroke rate can be as high as 3.2%/year if untreated (Olesen et al, Thromb Haemostat 2012)."
mdcalc.com/calc/801/cha2ds2...
Steve
Thank you for the link Steve.
It's important, I think, to be clear that the author and originator is explaining that a score of 0 in the old, outdated Chad2 system could not be considered low risk and therefore couldn't differentiate between those who need anti-coagulants and those who do not, whereas a score of 0 in his Cha2ds2Vasc system, which we all use now, IS considered low risk and not requiring, as he puts it, anti-thrombotic therapy.
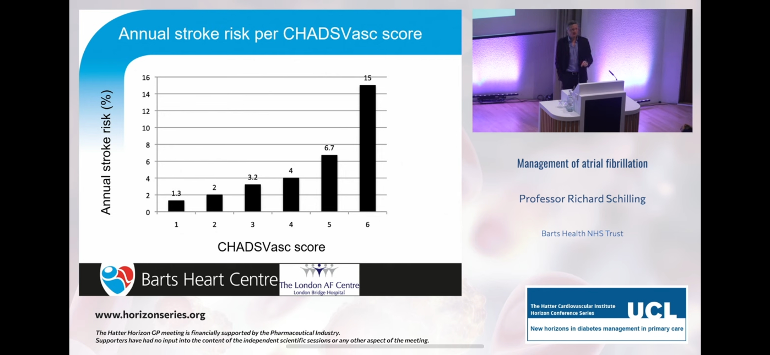
I’m pleased that you posted this because as soon as I saw the video I was perplexed. Professor Schilling is meant to be top doc but this explanation left me somewhat confused. I did think scare tactics were at play, and the presentation was sponsored in part by Astra Zeneca.
He is saying that if you aren’t anti coagulated and have a ChadsVasc score of 2, but haven’t had a stroke in 5 years, then in the sixth year your chances of a stroke are 1 in 10. The chart he presents is quite frightening.
If the cumulating is indeed correct as presented, then someone who doesn’t know that they have a ChadsVasc score of 2 at the age of 50 has a 50% chance of stroke in their 75th year. This rises to an 82% chance of a stroke in their 85th year ( ChadsVasc automatically increases by one at age 75). Surely the NHS would be all over the aged population giving out ECG’s (2 minute Kardia at your GP’s?) . Maybe they are and I don’t know about it.
If untreated and the ChadsVasc score is 4 at the age of 65 then accumulation leads to a 100% risk of stroke in a year by the age of 84.
So every female in the population with high blood pressure and diabetes ( or vascular disease) and untreated AF at age 65 will have a stroke by age 85. Really? 100% risk of stroke! What am I missing here.
Lets not even go where the ChadsVasc hits 6.
Hi
Um.... no that is not correct. If you had a stroke 5 years ago and have not had one since you are unlikely to have one. With AF the odds mount up if you are not on anti-co.agulant. At 70-80 it is recommended that your dosage be lowered. PRADAXA has 110mg and 150mg x twice day.
Research tells us now that if you have cancer in your body you should not have an anti-co.agulant.
Last week told in report I have a CHAD score of 5. Risk is 12.5%. I am at 4 years post stroke but mine was caused by thyroid cancer which caused AF that caused the clot and stroke.
Get your AF controlled and live your life.
cheri jOY. 74. (NZ)
Sorry but that is a nonsense response and please don’t tell me to get my AF controlled
I agree it is really confusing. The person I asked is a professor of statistics but I didn’t really come away any the wiser, except the headline that the risk does accumulate. But ask you say, it doesn’t accumulate to a certainty and that is the confusing part.
My understanding is that even with a 0 Chads score there is still a risk of a stroke as it never falls to 0% regardless of age. (even babies can have a stroke) But I'm not a statistician or Doctor.
All the best.
Roy
You are right. As I understand it ChadsVasc is a measure applied to AF sufferers only, not the general population. So. ChadsVasc score of 0 is still an AF patient (male under 65) but not necessarily worthy of anti coagulation and therefore at the same risk as the general population?
I don’t know, it just seems to be getting more opaque by the minute, fighting through the statistics. When I put my logic to the data given by Prof Schilling I come up with daft results like a 100% stroke risk.
Inherently I know it must be wrong, so then the question of accumulation queried by Sixtyslidogirl must need some sort of manipulation to make it fit the real world.
You are correct. I have a CHA2DS2-VASc score of 0 but that just means I am low risk rather than no risk!
Hi goosebumps. Risk is measured against time. The accumulated risk of say 20% over 10 years only applies as you stand there at the start of year one. So it is a projection of total risk over the forthcoming 10 years. If you do not have a stroke in year one then you risk over the remaining 9 years is 18%. At the end of year 2 it falls to 16% over the remaining 8 years etc.The chadvasc score will give a loading for risk to a given population, say male age 65 with no further comorbidities. There will always be variations in outcome for all individuals within the popultion group. If you remain stroke free you are likely to be at the healthier end of the spectrum for your peer group. A risk calculculator will basically give the mean average outcome for the group.
I am mindful of an expaination given to me by a teacher .when I was at school.
During WW2 the probability of death for a fighter pilot during the Battle of Britain was 1 in 20 per sorte. Statisticly most pilots would not survive 20 flights. 20 times 5% equals 100%.
This statistic only applies as the pilot goes out on his first flight and is a projection of the forthcoming 20 flights. At each flight the risk is still 5%. At flight 20 the risk is still 5%. Intuitively one feels that the risk increases with time, ie your luck will run out. However at any one point in time the risk is static at 5%.
All the flights are independent events and as such the risk per event does not change.
Regards
That makes more sense to me.
Hi
If you have had a stroke or TIA your CHAD score will be 2.
I was 70 at my stroke time, add on 1 for female, add on 1 for over 65 and then add on 1 for AF.
So my Cardiologist tells me last week that at CHAD 5 and 4 years down the track and on PRADAXA 110 x twice I have a Stroke risk of 12.5% in my life.
If you have had a stroke I would suggest you take an anti-co.agulant at any age.
Your risk of blood clots with AF add to that.
cheri JOY. 74 (NZ)
There is no doubt about it, probability can be very counter intuitive as this thread demonstrates. For those who might be interested look up the base rate fallacy, the prosecutors fallacy and the Monte Hall problem.We can all forgive ourselves when we become confused when trying to understand statistics.
If anticoagulants reduced the risk of stroke and didn't have any potential negative side effects then everyone would probably be on anticoagulants. However, being on anticoagulants could have dire consequences if you suffer a major bleeding event. So your doctor has to weigh up the risks and decide on balance, whether to give you anticoagulants or not. That's where tools like CHA2DS2-VASc and HAS-BLED are used to assist decision making.
Not what you're looking for?
You may also like...
Stroke risk
A question to throw out there - if being over 65 and female gives you a Chads of 2 and deems you...
Stroke risk
Trip to A&E after a bout of severe irregular heart beat.
Having suffered from AFib for several...
Stroke Risk
I find the charts they calculate your risk of a stroke
Worrying.I am on Blood pressure tablets...
Some good news about stroke risk
Thanks to the member Quest4NSR and his post "Great video", many of you will have to change your...
Stroke risk?
My CHA2Ds2-VASC score is 0, but I think I'd prefer to take an anticoagulant (probably Apixaban)....