It is based on 3,478 consecutive patients operated upon by Dr Catalona from 1983-2003. PSA testing did not become prevalent until the 1990s, so the high number (32% 10-yr BCR) is not surprising.
It is based on 2,516 patients treated with RT at Cleveland Clinic. The abstract doesn't give the dates they were treated, but with 78 months median f/u, we can be pretty sure that some were diagnosed pre-PSA and few or none received doses of radiation now considered curative or with the duration of adjuvant ADT now known to cure high-risk patients.
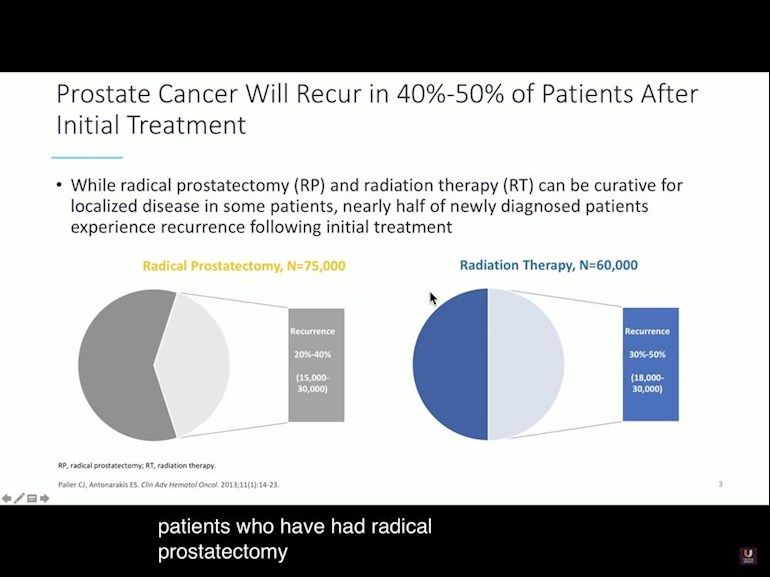
Looking at it again, and with the benefit of reading one of the studies you linked, I think the slide may be a little misleading? A casual glance might lead one to believe the slide represents 75,000 study patients who underwent RP...thus the 20-40% would be the range of results from different studies totaling 75,000 men. However, you are pointing out that the 20-40% is based on smaller numbers from a much smaller population. I would think Hopkins and others now have updated numbers for men who underwent treatment post 2000?
In 2019, Dr. Klotz presented this graphic....... well, I guess we can't paste fotos with the healthunlocked system? and I see no way to attach an image when replying...only when posting, and then a limit of one?
and of course, any numbers are only useful in practice when other patient characteristics are enumerated.....for example the Hopkins nomograms.
For RT, modern 10-yr biochemical recurrence-free survival (bRFS) rates are around 95+% for low risk, 80-97% for intermediate-risk, over 80% for high-risk patients using brachy boost therapy, and 70% for very high-risk patients using brachy boost therapy.
I have no doubt that those bRFS rates will improve markedly when PSMA PET/CTs become the norm for screening unfavorable risk patients (instead of bone scans/CT).
Now that we all use the NCCN risk stratification system, no one would publish "global" numbers like you posted anymore. The mix of risk affects the BCR rate as does the year they were treated and the treatment modality.
Yes! Just an example of what even some Docs have been publicizing not too far in the past. I'll start another post, just so I can attach foto of Klotz's treatment comparison
Because it used to be the case that men only got biopsied when they became symptomatic. By the time a man has symptoms of prostate cancer , it has spread so that local treatment is no longer curative. With the advent of PSA tests, it became possible to biopsy and treat while the cancer was still only in the prostate.
(1) See my post above
(2) 100% - there is no data indicating that it can be cured.
I checked the Phillip Koo video. He was making the point that in the olden days, when only bone scans/CT were available, many unfavorable risk patients seemed to have localized prostate cancer. Because the sensitivity on bone scans/CT is so low for detecting metastases, many men received radical prostatectomies or radiation who wouldn't have if it were known that their cancer had already metastasized. All of the men with undetected metastases had recurrences. Now that we have better PET scans, we have the opportunity to get lower recurrence rates because those men will be able to avoid radical treatment (except those who are oligometastatic - but for them, no one expects treatment to be curative).
His video was about patient selection using PET scans, not about treatment.
The question is how long until the insurance companies get on board. My Drs fought for a Axumin scan because of PSA 156 but it was denied. I would have paid out of pocket but the Drs said it would not have changed my treatment so I should not pay the money. I wonder about that now but its the old if I knew then what I know now, I would have paid for it for sure.
I agree. Axumin was only FDA-approved for recurrences after treatment. The new PSMA scan is approved for men with unfavorable risk prostate cancer too. So far the cost is about $3000 at UCLA and UCSF and Medicare and insurance haven't yet agreed to cover it. I'm hoping they will in the coming months.
So, actually, for those men, it wasn't recurrence anyway......something can't "recur" if it was never removed/killed by the initial treatment....it was actually cancer not targeted by whatever initial treatment. I broke down and bought Walsh's book today...haven't gotten to the chapter on details, but so far what I have read seems to point to the benefit of primary treatment, surgery or radiation, even for advanced cancer...."debulking" the primary tumor.
I respectfully disagree Allen! If all men diagnosed read his book before treatment decisions, many men would have a much better understanding of their choices and what to expect.....and I don't think it makes sense to disregard the contributions from a number of highly credentialed Hopkins' professionals and others from other institutions, as well as, of course, a man who has dedicated his life to the profession. The book is the 2018 revision. Most men will never dedicate the time you have to researching the subject.....indeed, most men do little/no research IMHO. I have a good very intelligent friend, both parents were MDs and wife a sharp NP, and he thinks I am nuts to spend my time on this and not simply decide on a Doc I trust and go with his/her advice. I've found that to be the thinking of most folks who have dealt with medical problems, including PCa.
This would be something good to post each time update is available. In teresting, my Kaiser Uro mentions NCCN.....but Kaiser doesn't use the guidance for PSA cutoff...they use age-adjusted numbers...eg 4.5 ages 60-69, 6.5 age 70+ ?? NCCN says consider MRI pre-biopsy, but Kaiser allows only if some troublemaker like me asks for it.....and then denies subsequent fusion biopsy??
Yes, I see that NCCN suggests PSA of 3.....but that may be too high for a man of age 40-50? My Kaiser Uro considered my increase from 4.1 in mid 2014 to 6.6-7.5 in last two years(now age 72)...even with my regraded MRI, from PIRADS 3 Kaiser radiologist to PIRADS 5 OHSU radiologist, he. Kaiser, said still not convinced I have "serious" cancer. As amateur, PIRADS 5 terrified me!! two radioligists disagreed on prostate size.....one calculated 81CC, the other 95cc. My PSA density is low with either measurement..if that mean anythings> the lesion in transition/anterior zone is approx 1.5 cm cubed......5/8" cubed. No other alarming things seen on MRI ...as far as cancer goes. Does his "not convinced " remark make sense to you?
I'll ask re the PHI....but having a biopsy makes that unnecessary?? Since cancer is a terrifying word, most friends a nd relatives think that I'm doomed because I haven't already had a biopsy! Without Google, I'd probably just done whatever the Doc advised.....ie no MRI...but he admits he would have probably missed the lesion, since not in peripheral.....so I would have faced multiple biopsies probably.....I wanted to avoid that scenario!! My bad experience "validates" my concern about multiple biopsies!
Silly people exist. My mpMRI reader estimated my prostate's volume to 59.465 cc. Yes, "accurate" to the 3rd decimal digit. From this alone, I could tell that he/she was totally incompetent for this job. I did a numerical integration across the relative MRI prostate sections/slices and ended up with a more modest volume of 40 cc. Did the same with another CT and ended up with 54 cc. It is a very widely known fact that the ellipsoid's formula they are using for the calculation is far from being accurate, as the prostate has more of a pear-like shape than an ellipsoid. There are software packages that automatically do what I manually did, but who cares.
No surprise, after prostatectomy it was measured at 35 cc!
PHI can be used to avoid an unnecessay biopsy and can be used for tracking for AS, instead of PSA or % free PSA. PIRADS just means "very suspicious." My friend had a PIRADS 5 where no cancer was found and no PIRADS score where some GS 4+3 was found. There is high inter-observer variability. Your PSAD is a good sign.
I'm a bit confused - have you had a biopsy with sedation yet? I had a biopsy with sedation at Kaiser in Sacramento many years ago - so they do them. I would assume they can use propofol now.
Thanks Allen...no I haven't> Kaiser uro said he could do sedation in an operatory, but he doesn't have the fusion equipment....so he said, were it him or a relative, he'd advise having the fusion biopsy at med school......to assure we had the highest confidence level in the results. He was confident in hitting the lesion.....if it was visible with his US equipment....no guarantee of that of course. Perhaps the lesion being in anterior/transition zone also influenced his thinking.....I'll be talking to him in a few days.....we can either ask Kaiser to approve a redo at OHSU with sedation, or take our chances without fusion at Kaiser?. ...I found one study where supposedly fusion biopsy averaged 0.3 cm miss of center of lesion, whereas cognitive average was 0.7 cm. Your friends are good examples of why combination targeted and standard TRUS biopsy, common sensically, finds more significant cancers than either alone. A meta-analysis summarized it this way....... when there is a target in 100 patients, on average standard biopsy finds 34 significant cancers, targeted biopsy finds 39 cancers, and the two together find 44 !! I looked at 12 biopsy naive 1st biopsy studies , and found that, on average, combo biopsy found 25% more cancers than standard TRUS alone, and then, as you stated, MRI misses some lesions, mostly the small ones I believe...and there is also problem of grading. Still, I don't think we can dismiss added value of prostate MRI.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.