also what does "cumulative incidence" shows? Is the total percentage of people that progressed?
Can someone explain to me the below graph? I wa... - MPN Voice
Can someone explain to me the below graph? I want to understand what is the total percentage of "true"ET progression in these 30 years.
Written by

Aneliv9
To view profiles and participate in discussions please or .
16 Replies
•
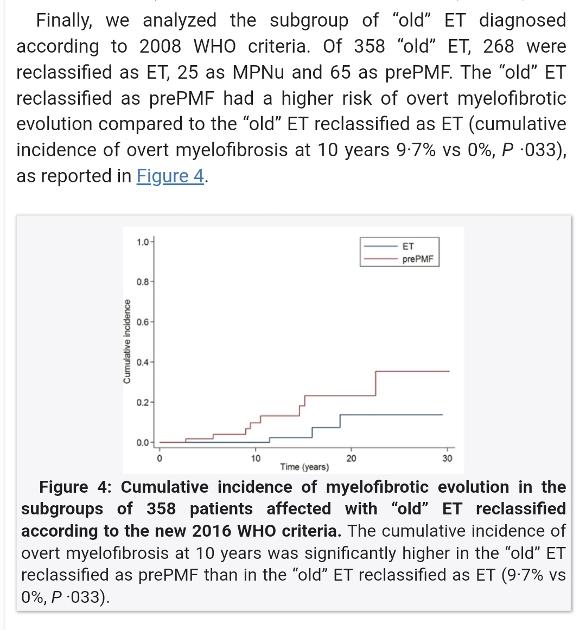
This study separated Pre-MF ET from ET using current standards. Pre-MF ET was not well known until recently. If your DX is Pre-MF ET the prognosis is higher for progression (the red line) If it's ET this study found no progression at all over 10 years. This study does show just over 10% with ET progressed at 20-30 years, with Pre-MF ET being at upper 30's%.
Cumulative is adding each case as they occur, the stair steps seen in the plot. So one case at 3 years gets added to another person progressing at 5 years for 2 total at that point. This is different from a "rate", just for example, of 2 cases per year. 2 cases per year would ac"cumulate" to 4 cases after 2 years, 6 cases after three years....
From the IFN studies, the best way to stay on the good side of these odds is by IFN therapy, if suited for each of us.
Thank you for helping me get an idea. So in the above graph, can we say that in a "total of 30 years 10% of the total ET cohort progressed to MF"? And one more question if you know! This 10% percentage is the highest percentage that shown up, or the average/promedio?
More accurate would be "at 30 years" but you've got the idea.
The ET value actually looks closer to 12%, but it's hard to read without their actual data.
It is not a highest or lowest, but an actual number they measured in this study. But your point on highest etc is relevant; there are likely other studies on this area with different numbers. Most likely these would have at least somewhat different results, as is normal.
There is another item to consider, most studies as they get to very long times, have patients leaving the study. So results at the longest times have fewer subjects and may be less reliable than the earlier year results with more participants still in. The long straight lines at 20-30 years suggest this issue to me. In these things more is better.
So do you believe this is the case and in this study? 16% fibrotic progression with median follow up of 13 years (0-47 years). So i am wondering.. How can i estimate the probability of progression in a long time course (40-50years)?? It is possible to be even as high as 40.or 50% if in some studies that i have seen the 20 years progression is 15%! I really looking for some answers cause I can't put my mind at ease..😟
If the chances of progression are in the range of 15% at 20years, it looks inevitable to progress in the next let's say extra 40 years. Isn't it a known life time risk (let's say 50 years)?
S
This was a different type of study that the one above so they are not readily comparable. The phone screen shot also does not have enough info to figure it.
Yes it is i think the longest time study. It is not the same as the other one. A question is: if these studies give the MEDIAN follow-up time, doesn't this mean that half of the patients followed up for the above half range of time? Or they can also some patients leave the study and mess up results?
Also you can open the above image if you click on it (i can).
The most important missing topic here for younger MPNs is in 20 years the treatment options will have things we can't even imagine right now. The explosion in gene tech that is benefiting all cancers will do the same for MPNs. We're seeing just the start.
For us over-60's we should get some of it, but therapies avail 10 years from now are likely already known to us in early development, unlike the unknowable ones 20 years out.
What age are you now? I don't know how old the people were in the study. This makes a big difference. The development of MPNs, particularly MF is often found in older people. So a proportion of these will die of other things and won't be able to progress in eg 25 years which will account for EPguy's statement of many people leaving the study
I am 39 years old and i believe i have ET for at least 20 years. For younger age group (under 40) the risk is 16% in a long duration study. But i really don't know if all these are accurates if people living studies after a long time as EPguys said. I am really scared, cause triple negative status put me at high risk for AML if i progress to MF (3 out of 4 get AML)
I feel I am in a similar boat as you, I am 27 with ET. Good chance I will likely develop MF at some point in my life. I am hoping as all are we get a cure like hepatitis. But, regarding AML, there is some promising stuff happening right now with crispr. There is about 7 or 8 clinical trials running with crispr technology, so people are trying and working on a “cure” for AML. I would suggest following the trials. Maybe it will put you at ease as crispr gives a ray of hope that can likely cure MPN altogether. It is still an unknown how far of this all is but, it is moving very fast in the right direction
Have you found immunotherapy (such as crispr) being studied for MPN derived AML? It seems to be a distinct category of AML.
AML is still a rare MPN outcome, and with deep gene sequencing the risk of it is getting more quantifiable.
From what I can find, the treatments for "conventional" AML are not usually effective for MPN derived AML, see sample report here, but if you have examples that's great to know.
The reports indicate SCT also may have reduced success rate for MPN AML, I'm not sure about this part, but SCT is the only effective treatment for MPN AML. My take, based on reports we've discussed in other threads, is with high risk MF, one wants SCT when it's clinically available. This is consistent with current thinking on MF, if one is an SCT candidate, do it before response to conventional MF therapy declines.
--
Immunotherapy is in early studies for CALR mutated MPN and early info is promising. For Jak2, there are currently barriers to direct use of this new method, but work is ongoing to unmask the Jak2 for use of immunotherapy.
--
MPN derived AML:
<<the co-existence of underlying MPN further complicates the clinical management (of MPN AML) and makes response to treatment according to standard criteria (ELN 2017) quite rare and short-lived when occurring.>>
ncbi.nlm.nih.gov/pmc/articl...
So if doctor see that an MPN starts to progress to AML ( i imagine some blasts will start rise up??) can't have a good result with a SCT?
From the overall info I've seen and posts we've had, if one is high risk MF, discussing SCT with Dr is warranted. Waiting to discuss SCT till MF is no longer responding to therapy, and by implication having rare progression to AML, is not best practice.
There is a report on this in prior posts, but I don't have it handy right now.
If I were to progress to MF I would proactively discuss SCT with Dr when/whether I should have the procedure. But absent high risk MF, I'm happy to work with the marrow I've got.
Is a stem cell transplant something you can talk to your haemo about?
Stem cell transplant is not offered as an option in ET