After surgery and salvage radiation therapy (SRT) have failed, it appears I'm headed for androgen deprivation therapy. Like many things in the world of prostate cancer, the recommendations as to when to start ADT seem to be all over the place, so I'm seeking any insights folks may have based on your own experiences.
Background
Nov 2010 — Diagnosed at age 52. Routine physical exam revealed palpable mass during DRE. PSA 5.0. Biopsy revealed Gleason 3 + 3.
Jan 2011 — Radical prostatectomy. No seminal vesical or lymph node involvement; no extra capsular extension; negative margins; pathological Gleason 3 + 4.
Sep 2015 — PSA went from undetectable (<0.03 ng/mL using this lab) to 0.05 ng/mL. PSA bounced around between 0.04 and 0.08 for about 18 months.
Jul 2021 — PSA hit 0.21, passing the traditional definition of biochemical recurrence of 0.20.
Nov 2021 — PSMA PET scan at PSA 0.23 ng/mL; negative for prostate cancer.
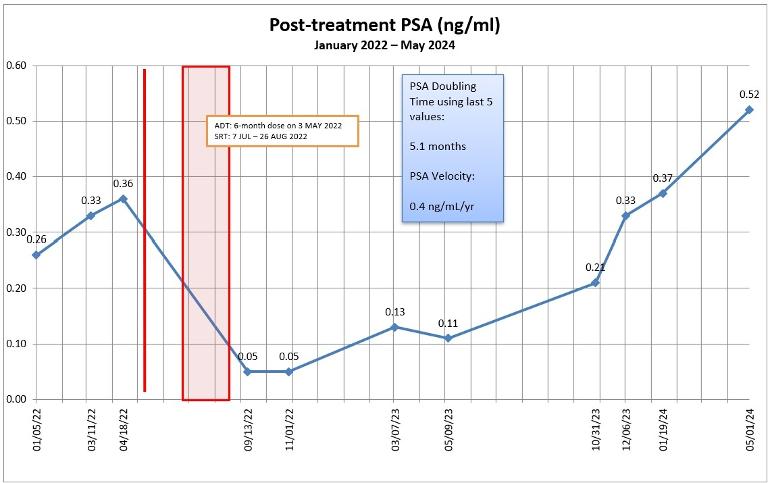
May 2022 — Received six-month dose of Eligard in advance of SRT. PSA 0.36 ng/mL.
Jul – Aug 2022 — 35 sessions of SRT to prostate bed only; 70 Gy.
Nov 2022 — PSA 0.05, mainly from effects of Eligard.
Mar and May 2023 — PSA 0.13 and 0.11 respectively.
Oct and Dec 2023 — PSA 0.33, 0.37, respectively.
Jan 2024 — PSMA PET scan at 0.37 ng/mL; negative for prostate cancer or metastases.
May 2024 — PSA 0.52; PSA doubling time dropped to 5 months.
What's Next
In February, I met with a medical oncologist for the first time (when my PSA was 0.37 and just had a negative PSMA PET scan). In a nutshell, her thoughts were to wait about 6 months (August 2024) and see what happens with the PSA and to repeat a PSMA PET scan to see if we could determine what was really going on. If the scan revealed lesions, then we might be able to go back and zap them with additional radiation therapy.
She was also inclined to delay the start of ADT until my PSA hit 2.0 ng/mL, and she was thinking it would be just ADT and not a combination therapy with an antiandrogen. We really didn't get into the discussion as to whether it would be continuous or intermittent ADT.
Research
Here are three research papers that I've come across addressing this topic.
I'm going to reread them, but my general take-away was that there wasn't a general consensus on the timing or the benefits of early ADT.
Questions
I have an appointment with my urologist on 14 May 2024, and I'm sure we'll discuss this in detail then. For the group:
▫ Does starting ADT early delay metastasis?
▫ If ADT is started early, will that make the cancer ADT resistant earlier?
▫ Aside from not experiencing the ADT side effects, is there an advantage to delaying the start of ADT?
▫ Is there a PSA threshold at which ADT should be started?
▫ Is there a PSA doubling time threshold at which ADT should be started?
▫ Any advantages to continuous vs. intermittent ADT?
(Yes, I realize that every case is unique and that very few of us in these forums are medical professionals. I just value insights gained from others' experiences.)
Summary
While I tolerated the six-month dose of Eligard pretty well, I'm in no rush to start ADT. My inclination right now is to wait 2-3 months and get one more PSMA PET scan done to see if it can finally reveal what we're dealing with before starting any further treatments, whether it be more radiation therapy or starting ADT.
If you've made it this far, thanks!
Written by
dans_journey
To view profiles and participate in discussions please or .
Hi Dan, Rob here, I’m a follower of your in depth Blog too (one of the best out there), I've found these emails helpful for some in depth information, here is one:
There have been two clinical trials (PRESTO and EMBARK) that address your situation. They both gave short term ADT+ARSi to men with detectable PSA (0.5 and 1.0, respectively) and rapid PSADT but no detectable metastases on a bone scan/CT:
Thanks Tall_Allen I printed those for future reference. They may come in real use in the future. Unlike the OP my horizon is more limited and that makes decision making somewhat easier. Seems to me that at almost 80 a timeline goal of say 85 maybe realistically achieved.
If you have nothing better to do, just check my thread entitled: "An engineer's Bicalutamide maneuvers". I have no hope that it can shift your treatment from SoC by even a single millimetre, as you are in the US and only understand fractions of an inch.
key questions and have wondered the same. If one knows it is trending up, do you hang around waiting for pet psma scan to work or immediately do a burst of adt salvage radiation eg to prostate bed and lymphs then stop the adt after 6 months and wait to see if that was a “cure”? or do you wait until 0.2 and hope the scan shows where it is. It is stated that oet psma is hobbled by being on adt. So you gain one tool (a scan) and lose the other (keeping it in check).
That's the exact conundrum that I debated for the longest time. I really wanted to know where the cancer was located before we started zapping with SRT. That's why I went for the PSMA PET scan in November 2021, full-well knowing that, at my PSA level (0.22) there was only a 35% - 40% chance of the scan detecting anything. It didn't.
What prompted me to go ahead with the SRT was the fact that my PSA doubling time was decreasing at an accelerating rate. The consensus was that SRT is most effective when PSA is below 0.50, and mine had jumped to 0.36.
The radiation oncologist was on the fence about doing concurrent ADT with the SRT. After much discussion and consideration, we opted to do the six-month dose of Eligard 8 weeks before we started SRT on the theory that the ADT would "soften up" the cancer cells to make the radiation more effective.
Hindsight is always 20/20 and, in retrospect, I might have waited until the cancer showed up on a scan before deciding my next treatment step. But even after my SRT/ADT when my PSA hit 0.37 in January 2024, the PSMA PET scan didn't reveal anything.
One thing that I've learned in 13+ years of dealing with this is that very little, if anything, in the world of prostate cancer is cut-and-dry, and that the best we can do is educate ourselves and make the best decision possible with the information at hand at the time.
I have a similar journey. Not sure where I stand right now. After RP, about a year later psa rose, my primary talked to me about radiation as the urologist who did the RP left the State. I was sent for radiation, also given 3 month shot of eligard. 33 radiation treatments to the prostate bed. Psa went to zero for the first time (post surgery it was still low but not zero). About a year after radiation and ADT, psa started to rise again. Have been with RO during this but but asked to meet with a Medical Oncologist (just met him) said velocity was slow and he would prefer to wait since the first (before radiation) PETSCAN did not show anything. Your psa is certainly rising faster than mine, mine is about .02 per month. One issue I had with the Eligard was after a month or so I needed supplemental oxygen since my O2 would hover at 80 or 81. Once my Testosterone went back up and the hot flashes stopped my oxygen went back to normal and have mot needed oxygen since. I am 57 and never had oxygen issues before. (Shrug) it seems like RO and MO are on the same page regarding checking and Scans. I hope they know what they are doing. They both have said since my Gleason was only 3+3 and no spread (except for perineural invasion) I should not be having any issues. In all honesty I hurt everywhere and am a little tired even doing small stuff around the house. Both doctors say they think that is not cancer related . Good luck. I think you will do great. This is a weird journey.
Not to mock you but to be realistic...... I too suffer from some of the same Pca symptoms that plague you but I'm 87 years old and have been fighting those tiny mother fuckers for 22 years. Of course, find out what can help you NOW and live until you're 90. (Note: I still don't know why I'm still around, luck maybe?).
Thanks, John. I know that I still have plenty of years ahead of me on whatever treatments we decide. And, barring any other issues, I'm sure that I'll still be around at the 22 year mark. (I'm 66 with almost 14 years since diagnosis.)
"... After surgery and salvage radiation therapy (SRT) have failed, it appears I'm headed for androgen deprivation therapy. Like many things in the world of prostate cancer, the recommendations as to when to start ADT seem to be all over the place..."
My MO did not believe I needed ADT after radiation at age 78. Nor did that MO or the Urologist who was handling my follow up insist on ADT after PSA had double twice and a scan showed residual in the prostate and metastisis to one node. ADT was held out as a last resort. The Urologist suggested pelvic radiation might avoid ADT, so I did that and the PSA did drop.
After the PSA started doubling again, I insisted on ADT. But the Urologist said no hurry, wait until we can see where the cancer is. So a second scan showed it was growing in the prostate, almost gone from the radiated pelvic node, but now appeared in an abdominal node.
So finally I got on ADT with Orgovyx and Abiraterone. What did I gain by postponing ADT for 2-1/2 years after initial treatment? I gained unsalvageable cancer in the prostate and mets to two nodes. And as to the dreaded effects of ADT? I hardly notice.
Thanks for sharing your experience. My MO, too, didn't seem to be in a rush to get me started on ADT during that initial consult (before my most recent PSA test this week; he opinion may change now with that result in).
It was two years ago this week that I received my 6-month dose of Eligard in advance of the salvage radiation therapy. I seemed to tolerate it quite well. Mild to moderate fatigue and some hair-triggered emotions seemed to be the worst of it. No weight gain or hot flashes.
It will be interesting to see what the team recommends going forward.
I'm on mono enzalutimide (Xtandi) per the EMBARK trial. I'm not having any of the SEs that many complain about. In fact, I think as my T returns, I actually feeling better than I have in a long time. I was on mono Eligard prior to switching to mono-enzalutimide. I can only recommend discussing mono-enzalutimide with your MO to see if it's appropriate for you.
Thanks for the recommendation. I had a six-month dose of Eligard before my SRT and tolerated it better than most. Some fatigue and hair-triggered emotions, but no weight gain or hot flashes.
I just read a post of yours from 2 years ago and I would like to follow up on your input to Just4Answers. At that time the discussion was to improve exercise to reduce fatigue SE.
Have you changed your resistance and aerobic exercise training long term? If so what effect has it had and do you today continue with that program?
Hi Mgtd. I have to admit that I didn't get into a great routine after the SRT ended in 2022, but one of my goals this year was to get active. So far in 2024, I've been averaging between 3 and 4 miles a day on brisk walks, and they've had a positive effect on my energy level. I've not focused on resistance training yet.
Yes many questions have no definite answers. I have had BCR after RP and salvage radiation with Short term ADT (similar to spport trial). If I have second BCR, I will be in your exact situation.
My expected plans at second BCR at this point will be to wait till PSA hits .5 ng/mL for a PMSA scan. If negative at .5 ng/mL, I will probably let it go to 1 ng/mL and rescan (assuming Insurance approvals). I don't know if there is a "sweet spot" to allow the PSA to rise without incurring some risks of spread. PSADT will become a factor also. My goal of letting PSA drift up until site of recurrence is identified is to use spot radiation to "sterilize" the lesion(s) of recurrence while I am oligometastatic. Then I would opt for concurrent treatment with ADT and ARSI for 36 wks (embark trial)
Thanks, FlyJ. I'm of a similar mindset to you at this point—let the PSA get to 0.7 to 1.0 and do another PSMA PET scan and go from there. We'll see what the medical team suggests when I meet with them on the 14th.
Seems for both of us our RP and salvage RT to prostate bed failed to get all the cancer. Also, gratefully, it seems our remaining cancers are not fast growing and fast spreading.
Regarding "Nov 2022 — PSA 0.05, mainly from effects of Eligard". Might this suggest your six months of Eligard indicates you are CR? I would have been looking for/hoping for <0.010 on ADT - as I was after my salvage ePLND nadir of <0.010 and then year on bicalutamide for added insurance.
I have had three clear PSMA PETS, two Ga68 and Pylarify, all done at or below PSA 0.11- raises question is my cancer PSMA avid, especially as the FERROTRAN nanoparticle MRI identified pelvic mets at 0.11 whilst the corresponding Ga68 was clear (yes a low PSA for PSMA imaging but the nanoMRI indeed identified pelvic lymph node mets).
My next imaging coming up in July is an mpMRI and fluciclovine or Mayo's Choline instead of PSMA.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.