This has been covered in some form before. But I came across this report that summarizes misc info from Cornell in a nice clean manner. See link, it's easy reading.
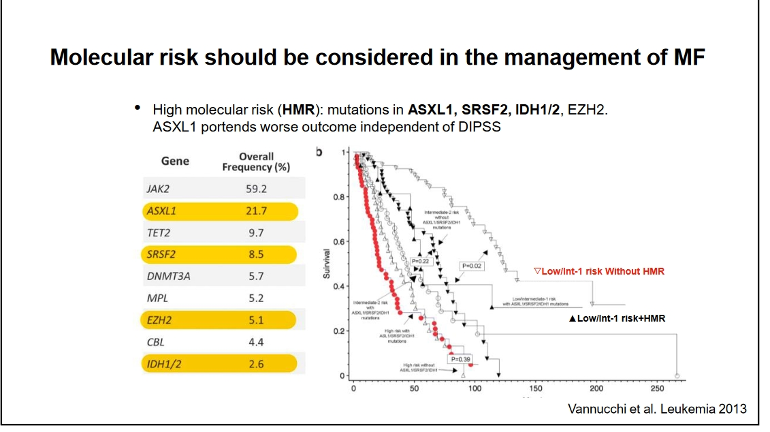
A specific takeaway is with the high risk (HMR) mutations in yellow here they lean toward SCT (stem cell transplant) if possible rather than waiting. See #1 guidelines below. There's also a good plot, slide #30 in the report, of the survival benefits of SCT vs various risk levels.
-Note that TET2 and DNMT3A are not in the high risk category with MF. But high risk ASXL1 is most common non-Jak2 in MF (22%).
For MF they recommend INF for lower risk earlier MF, at low doses, see 2nd set of guidelines below. Low doses is different from the current PV practice we see, maybe because of over reductions of some blood counts with INF+ MF.
--
For PV most info is familiar, but buried on slide #20 is a note that Phlb increases risk of fibrosis. I don't recall this anywhere else, but it may be in the long term INF Cornell reports we've discussed.
--
There's also this statement <<First step towards optimal treatment is making an accurate diagnosis
Bone marrow histology is crucial!>> This has not been so clear in our posts and experience.
--
Another chart shows there are 1763 MPN trials registered now. We like that. USA has the most ongoing, 1200, (one supposed benefit of our outrageous drug prices) Euro is next at 429.
==
#1- Risk-adapted treatment guidelines for myelofibrosis:
• Low to intermediate-1 risk (by IPSS/DIPSS/DIPSS-plus score)
- Observation alone for asymptomatic patients
- First line HU for symptomatic splenomegaly
- Ruxolitinib for highly symptomatic splenomegaly or constitutional symptoms
- consider Interferon (rIFNα)
• Intermediate-2 to High risk (by IPSS/DIPSS/DIPSS-plus score)
- Allogeneic stem cell transplant (SCT) for eligible patients
- First line Ruxolitinib for splenomegaly
==
#2- INF for MF:
What about Interferon in Myelofibrosis?
WCM experience:
- IFN should be used at low doses for sufficient duration (>12mo).
- Patients who are most likely to benefit are those with:
Great report - thanks. Interesting on their call for BMB. My MPN specialist agrees completely and almost "requires" his patients to have a BMB for definitive diagnosis, additional information (which is why he tries for the NGS panel as well) and to establish a baseline for potential future changes (almost as he would never push a patient to have a BMB that was against it but strongly encourages the procedure to provide additional information even if it will not immediately impact course of treatment)...
Exactly- I was [slightly] PO'd at the radiologist who interpreted my Abd U/S for saying the I had splenomegaly, because it was apparent that he didn't account for my body habitus which is, shall we say, generous [6' 1.5" and >240#, less muscular than in my prime, but not totally gone to seed [yet]]
The bit about phlebotomy increasing fibrosis in PV patients is not the view of most experts, from memory the last news I heard was that it was not the case. If you look at that slide and that comment it looks like it comes from 1994!. I suspect that a lot of the info on the whole pack comes from the thinking and views of Dr Silver , as we know he is very Interferon from diagnosis , not a view other experts necessarily agree on. I hope this info is of some help you those who having read the slide may be concerned about venisecting causing fibrosis, to the best of my knowledge it’s not correct.
My haematologist also agrees with the view shared by many specialists that phlebotomies increase the risk of fibrosis as it induces a chronic strain on the bone marrow. It seems to make sense if you look at the average live expectancy of patients treated this way in the past, or the percentage of progression towards MF.
Thanks for the note on 1994, that is prehistoric to us more recent patients. The other date on the slide, 2020, I think refers to this Silver group report which we've discussed in various threads, including this familiar plot. This does show higher MF risk for pleb vs even HU and matches my memory that they found HU to be better than phleb only.
<<Phlebotomy is unacceptable as permanent treatment because of the poor clinical tolerance and the frequency of vascular complications. This treatment is also associated with a risk of early progression towards myelofibrosis with myeloid splenomegaly>>
This ancient one also reports 50% MFS at 15 years, which strangely is not way off the plot here at 60%. By comparison HU is at ~80% and INF at ~90%.
--
So there may be something to it, phleb is higher MF risk, I had not thought about it before.
Remaining question is bias etc to the data in this plot (and the ancient data). I actually asked one of the authors of the newer one about it and he said they tried hard to provide for the retrospective biases and the strong results also compensated. Also they have no HU bias and data showed it advantageous.
I can’t quite remember where I got the info that venisection doesn’t cause fibrosis. Prior to Covid I used to go to the conferences in Scottsdale with MPN foundation at Mayo and also the doctors one organised by DrSilver and Dr Spivak in New York, I also am on the MPN List forum. The last doctors one in NY I attended was in 2019 and it might have been there, Dr Spivak is believer in phlebotomy and I am sure it would have been debated by him as he has strong views. Things may have changed since then but I would have heard about it on MPN List. Common sense tells me that venisecting wouldn’t still be first line treatment in most countries if it caused fibrosis.Having said all that I might be wrong and keep an open mind. Dr Silvers graphs look convincing so I will as around re latest info.
thanks for posting that paper by Nature. Here is the only reference to the point under discussion in that paper.
"One may argue whether the conservative approach based on phlebotomy and aspirin only is adequate in low-risk PV [8], also considering that a cytoreductive therapy like hydroxyurea may reduce the incidence of thrombosis and the evolution to myelofibrosis compared to phlebotomy alone"
Note the phrase "one may argue", ie they are not saying phlebs cause fibrosis in this paper, saying one may argue is very different. This paper was July 2020 by Kiladjuin and Barbui. Kiladjuin is and always has been a fan of early intervention so I think if it had been proven phlebs cause fibrosis he would have said so.
Hi ainslie,The diagram above shows fibrosis in 50% of patients treated for 20 years with phlebotomy only, versus 15% treated with IFN. There’s therefore a strong evidence that phlebotomy only leads to earlier fibrosis.
Interesting the ref (9) on fibrosis in the quote is also from 1990's. But it points also to reduced fibrosis with HU. It's paywalled, but seems there are three reports toward HU-reduced fibrosis.
To clinch the deal some newer reports would be good, but I think the field has moved on so we might not see fresh ones. With the three separate ones here it is a strong trend HU lower risk than Phlb.
That's funny, I don't have a NY library card, but that authorization screen didn't even come yesterday.
So, anyway, today it did, but when I clicked on the "Search for another location" link- the 'paper' was there.
This was a highlight: "We already know that repeated phlebotomy is a purely palliative therapy that in addition induces not negligible disadvantages (iron deficiency, increase in platelets, increase in risk of myelofibrosis...). "
and
"We know that maintaining the hematocrit level stable below 45% over time is crucial to reduce the incidence of thrombotic events, a goal that is difficult to achieve with phlebotomy only. We know that Ropeginterferon therapy provides similar short-term benefits than hydroxyurea, but higher benefits in terms of molecular response. We perfectly know the safety profile and contraindications of interferon, a drug that has been used for decades to treat PV. The low-risk PV study now shows that Ropeginterferon provides clear advantages over phlebotomy for a surrogate of thrombosis, i.e., hematocrit. Is it the time to change our practice for so-called "low-risk" PV? Our response is yes..."
2019 is a long time ago for the latest thoughts, which seems weird. It would be curious whether Dr Spivak has adjusted any views in light of the final Ropeg data. I think many top MPNs are adjusting. On the Silver report, I believe they have no bias toward HU so the result showing superiority to Phlb might be onto something.
But it's likely there is a study showing phlb without fibrosis risk, we see diverse results in so much of our data. Best we can do is look at the trends and details to judge.
One strong trend and detail on another aspect I've posted is correlation of CHR to MR on INF. My Dr is not with it there yet.
So very right, I use "correlation" intentionally when I talk to him to note it's not proven. We're good on that. But I want to dose to CHR while he wants to titrate to a set number that well exceeds that measure. (I have very good CHR response to INF so far) I hope to see data that show improved outcomes (progression, MR, symptoms...) when dosed to exceed CHR, and/or a set number. I find only the three separate reports that show CHR --- MR. The Ropeg study dosed to CHR to get their reported median AB reductions and more than one study noted no correlation of MR to dose.
But you're right, we all would prefer to see causation demonstrated.
Hi EPguy,I wouldn’t worry too much about the way your haematologist wants to titrate your numbers as long as your quality of life is good. His job is all about tuning the hematopoietic system and he’s an expert, by definition. He’s got the knowledge we don’t have about this industry, and reading abstracts is not enough to make us knowledgeable enough. In my opinion, he should care about our signs and symptoms, and not so much about our limited understanding of statistics or histophysiopathology, etc…
Agree about QoL. That's why I worry. Sorry for long reply.
QoL is my motivation for not over shooting the dose. Dr & I do agree on going for AB reductions. We're in a good place together now as we communicate more in detail. I'm his 1st Bes patient so we agree we're both learning.
I've actually read these full reports on INF for CHR vs MR vs BMR in close detail. Much of this data is new and it's hard for anyone, incl Drs, to keep up on it, but it's right on the point for AB reductions. I'm super motivated and able to make some sense of the relevant parts. (I am weak on stats) I've discussed with him the info (in different form) in my posts here. 1st one here includes my original plot from data. He does like the data I assemble.
My Dr respects my admission I know near nothing about Hem but also my motivation and ability to learn of my particular condition and options.
This is one sample from the reports I posted on (3 separate reports have this general conclusion) :
<<In Fig. 3, CR correlated to MR: “...the chance of achieving CR is 15 times higher for patients with a reduced JAK2V617F allele burden…which links a reduction in VAF to clinical response.” ... “We did not … observe a relationship between the dose of PEG administered and the degree of clinical response.”>> Image here shows this tight CHR-MR relation in two ways.
In my case, based on what I've seen here and in reports, I have a good CHR response at low doses on INF. (75mcg Besremi worked at least short term as a lower CHR limit). 5-7% of patients in the Ropeg study were in this low dose category (<125). Since the Ropeg study used CHR for titration and got its MR result, I want to understand what indications, if any, should prefer diverging from the titration schedule used in the study. I think my relatively outlier CHR response might be confusing things.
Hi EPguy,In case your haem overshoot the dose he’ll modify the posology accordingly! I believe his practice is based on individual patients, not on statistics. Most studies are designed for research purposes, not so much for the real world of clinical practice. Therefore, I personally wouldn’t rely on statistics to decide which dose I should inject. As you said, quality of life is paramount. Haems know about interferon for about 40 years. Besremi is a mere Deluxe version of Pegasys. Certainly a bit more complex to titrate in the short term…or in the long term, but I suppose nothing extraordinary new for an experienced haematologist.
I've had some eye issues so I want to stay conservative and ensure I can stay on therapy. My QoL is also extra, inversely, responsive to dose and he's lately agreeable to this aspect.
My thought is to take advantage of my individual patient good fortune in blood response, in context of the unusually consistent evidence, to try a CHR response based titration. This has been standard MPN practice in other meds and INF studies. I don't need more INF right now to get there.
He may have evidence that dose beyond required for CHR gives better MR, I plan to ask about that next visit. But the only high n info we have is the studies, and these point to a different conclusion.
In the background also is indications that INF does not provide very long term responses, I've posted on this. I'm eager to see the Ropeg 6 year AB results, it's not being released so far, and a study I've posted on PEG showed flattening or reversal of AB at 7 years. - I have zero evidence here, but it could be that not overdoing the dosing early might preserve more response headroom for the future.
This is a complication of my inventor thought process, always trying to process the info into a sensible form. He does appreciate that at some levels.
Hi EPguy,As far as I know AB reversal at 7 years is purely speculative, as we don’t know if the injected dose of IFN where constant during that time on the cohort of patients. There’s scientific evidence that the longer you are on IFN, the better the results on the allele burden. We do know that some patients are on IFN for over 30 years and some get a complete molecular response after that time.
These are from the old post here which discussed it. It used PEG INF.
--
I agree on the 20+ year results from the Cornell report we've had posts on, that may be the best info. This one is more specific while n is considerably smaller.
They started with crazy high doses, 450/week, but quickly ended with more familiar doses 45-135) titrated for response and toxicity. The crazy hi likely was not helpful but being brief was probably ok, esp since their PV result tracks the Ropeg one closely for the 1st 4 years.
See 2nd replies for the 2nd plot. It's a good refresher for me to look at it again.
It shows a complete MR stays low. But non-complete trended up strongly after 6 years. Ropeg study stops where this one gets interesting, esp the PV result in next post. It is possible Ropeg will see a different result, as might higher n. (I have an interest in this being so) I hope they do publish the 6 year allele, the more they don't the more it gets intriguing.
I will have to re-read my recent readings, but I know that I saw a citation that said higher dose INF in PV could lead to an initial increase in AB, and only later a drop in same, but that low steady dosing caused constant and reliable decline in AB.
I think I have also seen a report with a slight initial incr in AB on INF, but most seem to show the decline. It's possible the early studies were with non-pegylated, for which dose control and adherence were difficult. The "steady" part of your note suggests non-peg prior since steady is the feature of Peged. I also recall that early MPN use of PEG INF followed Hep C practice with 180mcg/week of PEG being common. That is a high dose in current practice.
It might not be that phlebotomy actively 'causes' progression to fibrosis, but it certainly doesn't do anything toward preventing or slowing progress to that [eventually if you live long enough] certain endpoint.
But since phlebotomy does in and of itself reduce the risk of thrombosis [a common cause of MPN mortality], and thus prolongs life to the "live long enough" stage, I guess in that sense, it could be said to promote fibrosis.
That is a good point. It follows the broader concept that cancer is more common now that life expectancy is longer than 100 years ago. So MPNs used to be expire before fibrosis showed up.
With that, the same thinking goes, we need improved MPN (cancer) therapies to match our longer lives, currently including HU (if above data are correct) and INF.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.