This pinned post replaces our earlier reference post about vaccinations for those with CLL/SLL. It has been divided into four sections, presented as a pinned post plus three replies.
Part 1 - GENERAL ADVICE & INFORMATION is contained in this main post
Special thanks to Jm954 and PaulaS for their invaluable contributions to this and the earlier post.
VACCINATIONS FOR THOSE WITH CLL - PART 1
GENERAL ADVICE & INFORMATION
People with CLL have a weakened immune system and are more vulnerable to infections. Because infections can be a major cause of death in CLL patients, vaccinations to help protect us are very important.
More advanced disease and treatments can increase our risk of infection and decrease our response to vaccines so early vaccination, wherever possible, is best. Even at advanced stages of disease, there still may be a surprisingly good response.
When you are first diagnosed it’s important to do a ‘vaccination audit’ to ensure you are up to date with your vaccinations and you should aim to stay up to date with any boosters from then on.
Revisit your vaccination status before you start any treatment and aim to get any outstanding vaccines or boosters first. You should aim for a minimum of 2 weeks prior to any treatment.
SPECIFIC ADVICE FOR THOSE WHO HAVE BEEN GIVEN CHEMOTHERAPY:
"If inactivated vaccines are given during chemotherapy, they should not be considered valid doses and individuals should be vaccinated again after treatment. Revaccination of individuals after chemotherapy or radiation is generally unnecessary if the prior vaccination occurred before chemotherapy, with the exception of hematopoietic cell transplant recipients."
Kevin Y. Wang, Pratik Shah, Brandon Skavla, Fatima Fayaaz, Jeffrey Chi & Joanna M. Rhodes (2022) Vaccination efficacy in patients with chronic lymphocytic leukemia, Leukemia & Lymphoma, DOI: 10.1080/10428194.2022.2133538. Here is the abstract: tandfonline.com/doi/abs/10....
GENERAL ADVICE FOR ALL WITH CLL:
“Live” vaccines should NEVER be given to people with CLL.
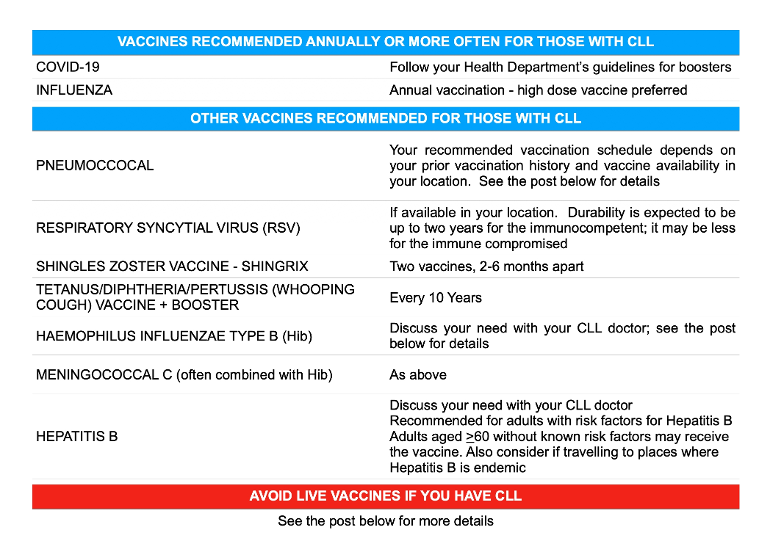
“Non-live” vaccines that are safe and advised for people with CLL include:
Influenza - Get the injected non-live flu vaccine NOT the live nasal spray
COVID-19
Pneumococcal - Some new vaccines have been produced recently that are more effective than earlier ones. If they are available in your country, you may need to self-advocate to receive them.
Shingles - Shingrix is safe NOT Zostavax
Haemophilus Influenza Type B (Hib)
Meningococcal C - often combined with Hib
Tetanus/Diphtheria/Pertussis (Whooping Cough)
Hepatitis B
Respiratory Syncytial Virus (RSV) - available through shared decision making in US from Fall 2023 for those over 60 healthunlocked.com/cllsuppo...
See Parts 2 & 3 for more information about safe vaccines.
Do NOT take the following live vaccines:
Chicken Pox - Varicella
Cholera - oral vaccine
Dengue fever
Influenza - FluMist a nasal spray usually given only to children is live; non-live flu vaccines are safe
Japanese Encephalitis Virus - Imojev vaccine is live; JEspect is non-live and safe
Measles/Mumps/Rubella (MMR)
Polio - oral vaccine
Rotavirus - Rotarix and RotaTeq are both live oral vaccines
Shingles - Zostavax is live; the newer vaccine, Shingrix, is non-live and safe
Smallpox - ACAM2000™ is live; JYNNEOS® is non-live and safe
TB - BCG vaccine
Typhoid - oral vaccine
Yellow fever
We may need to avoid people who’ve had live vaccines (eg children who’ve received the “live” flu nasal spray or people who’ve received the “live” shingles vaccine) as they may shed the virus. In the case of the flu nasal spray, this could be for at least one week up to two weeks - some medics advise 3 weeks to be on the safe side. healthunlocked.com/cllsuppo...
Always check with your haematologist in case there are other reasons why you shouldn't have particular vaccines. eg. when you are taking certain treatments or after certain treatments. It’s not that vaccinations are dangerous at these times, but they may not work so well. Note, though, that:
"People with severe neutropenia (absolute neutrophil count <0.5 × 10^9 per L) should not receive any vaccines, to avoid an acute febrile episode."
Some with CLL take prophylactic antiviral and/or antibiotic medication, the most common being valaciclovir or aciclovir to help prevent shingles. This is often prescribed to trial patients with a prior history of chicken pox or shingles.
A brochure for GPs produced by Oxford University Hospitals in the UK recommends "If a [CLL] patient has a history of shingles, then they should still receive lifelong Aciclovir as secondary prophylaxis in addition to the Shingrix vaccine."
The antibiotic Bactrim (a combination of sulfamethoxazole and trimethoprim) is also commonly prescribed to help prevent a certain type of pneumonia (pneumocystis-type).
Your CLL doctor is the best person to help you decide if you need these medications. Usually, they aren’t given unless you are in treatment for your CLL although some people continue them beyond treatment.
If you are prescribed an antibiotic or antiviral when you start your CLL treatment, be cautious about being taken off those prophylactic medications during or at the end of your CLL treatment. Many here have reported bad shingles or pneumonia episodes after stopping prophylactic medications, especially if they had a history of a previous, associated infection.
In January 2023, the US announced that Evusheld is not currently authorised for emergency use there and other countries that were using it have stopped. As of February 2023, Astra Zeneca is trialling another prophylactic, injected monoclonal antibody treatment for protection against Covid-19. We await further information about it and other treatments in development.
(Last updated April 2024)
CONTINUED IN PART 2- Vaccines recommended annually or more often
Written by
CLLerinOz
Administrator
To view profiles and participate in discussions please or .
The ideal time to get a flu vaccine is early enough in the autumn/fall each year to be just ahead of any flu wave in your area and late enough to maximise your protection throughout the season. The timing can be difficult so most people with CLL opt to get their vaccination early in autumn/fall soon after the vaccine becomes available.
CLL specialists advise some patients to get a second annual flu vaccine to extend their protection. Check with your specialist about this.
Different countries offer a different suite of flu vaccines before each flu season. Always avoid the live attenuated nasal vaccine, FluMist.
Safe, non-live vaccines are usually trivalent or quadrivalent (covering three or four strains of influenza). They might also be adjuvanted or non-adjuvanted.
In general, an adjuvanted vaccine has more ‘power’ than a non-adjuvanted one. Sometimes, the dosage of a non-adjuvanted vaccine might be increased to raise its efficacy. In that case, there might be very little difference between the non-adjuvanted and adjuvanted vaccines if they cover similar strains.
Now there are also cell-based flu vaccines as well as egg-based flu vaccines. At present, that difference is of most importance to those who might be allergic to an egg-based vaccine.
The general advice, then, is to get a ‘high dose’ non-live flu vaccine recommended for immunocompromised and/or older people. Be guided by your country’s recommendations. Links to UK, US and AU guidelines can be found in Part 4 of this post.
It’s also important that our nearest and dearest get an annual flu vaccine. They’ll get better responses than us and if they don’t get the flu, they won’t give it to us. In the UK, partners and carers are entitled to have flu jabs on the NHS. You may wish to ask for children to receive the non-live injectable flu vaccine to save the risk of them shedding the virus to anyone close to them who is immunocompromised.
For more information about influenza, its prevention and treatment in cancer patients, including in those with conditions like CLL, please read "Overcoming Barriers to Influenza Treatment in the Oncologic Setting" which you'll find on the Clinical Care Options website at: clinicaloptions.com/oncolog...
Antivirals are available for post-influenza treatment. Read this article for more information on that topic: theconversation.com/i-think...
2. COVID-19
Different parts of the world vary regarding what Covid-19 vaccines are available and this is constantly changing as new vaccines are approved.
Get whatever vaccine you can that you are scheduled to receive (so long as it’s not a live vaccine) because the best vaccine is the one you can get.
Currently, most people with CLL have received a primary course of 3 vaccines plus follow-up boosters. In 2024, the current vaccines are based on the XBB.1.5 variant of SARS-CoV-2.
The timing between doses varies from country to country but a minimum period of three to four months has been usual. Lately, that interval has been getting longer and six months is now more common for the immunocompromised. Be guided by your country’s recommendations. The immunocompromised often get approved for boosters ahead of the general population. Stay up to date.
Advice about when to get a scheduled Covid-19 vaccination after being infected with Covid-19 varies from country to country. In some, it's possible to get vaccinated once you've recovered from your infection and feel well enough. In others, there's up to a minimum six month wait. Check your country's guideline. The interval may be shortened in some circumstances (eg if you are starting treatment or before overseas travel).
You do not have to wait three months after being infected with Covid-19 to take vaccines for other conditions but should wait until you have cleared your Covid infection and have no fever or respiratory symptoms.
COVID-19 vaccines and myocarditis -Risk of myocarditis from COVID-19 infection is over 7 times that from COVID-19 vaccination. Vaccination risk is highest with Moderna: healthunlocked.com/cllsuppo...
In addition to vaccines listed in Part 2, the following vaccines are recommended:
3. PNEUMOCOCCAL
Guidelines for pneumococcal vaccination vary from country to country based on which vaccines are available.
Where it’s available, the recommended vaccine is Prevnar20 (PCV20). Vaccination is then complete.
Where it isn’t available, other possibilities include:
Prevnar15 (PCV15) followed ≥ 1 year later by Pneumovax 23 (PPV23 also known as PPSV23). Immunocompromised patients may be approved for Pneumovax 23 ≥ 8 weeks after PCV15). Vaccination is then complete.
OR
Prevnar13 (PCV13) followed ≥ 8 weeks later by Pneumovax 23 (PPV23/PPSV23) followed ≥ 5 years later by another dose of Pneumovax 23 (PPV23/PPSV23). Depending on your location, you might be considered for further vaccination 5 years after this.
OR
If you have had only Pneumovax 23 (PPV23/PPSV23) and no other pneumonia vaccine, you may receive one dose of either PCV20 or PCV15 (if available) ≥ 1 year after the last PPSV23 vaccine. Another PPSV23 is not then needed. Vaccination is complete.
OR
If you have had only Pneumovax 23 (PPV23/PPSV23) and neither PCV20 nor PCV15 is available, you may have PCV13 followed ≥ 8 weeks by PPSV23. An interval of ≥ 1 year is recommended before receiving PCV13. (Note that in some places the second dose of PPSV23 is not given after an initial dose of PPSV23 followed at least a year later by PCV13)
In some places, PCV20 may be recommended for those who have had PCV13 at least 5 years earlier.
See Part 4 for information specific to the UK, USA and Australia.
4. SHINGLES
The primary risk factor for getting shingles is a weakened immune system.
If you've had chickenpox as a child (the CDC predicts that over 99% of people born before 1980 have), then ZVZ can reactivate at a later date and cause shingles.
If it is available where you live, consider Shingrix. Do NOT accept the “live” vaccine called Zostavax. Shingrix requires two doses, with an interval of 2-6 months.
Some people report uncomfortable side effects from Shingrix, particularly after the second dose (although for some, it’s after the first), but they usually pass fairly quickly.
On the other hand, “about 10 to 18% of people who get shingles experience PHN (postherpetic neuralgia), the risk increasing with age.” “PHN occurs in the areas where the shingles rash was, even after the rash clears up. It can last for months or years after the rash goes away. The pain from PHN can be so severe and debilitating that it interferes with daily life.” Vaccination is preferable.
Apart from the terrible pain caused by shingles and the risk of ongoing PHN (postherpetic neuralgia), in 2022 research found that shingles is also associated with an increased risk of stroke and heart attack. brighamandwomens.org/about-...
As explained in Part 1 of this post, some with CLL receive prophylactic antiviral treatment to protect them against shingles.
From 1 Sept 2023 in the UK, Shingrix will be available to the immunocompromised from the age of 50 and above. It has replaced the live Zostavax vaccine and will also be available to the immunocompetent who are 60-79. See the links in Part 4 for more information.
In the US, Zostavax is no longer available. Shingrix is the standard vaccine on offer there.
In Australia. Shingrix is now available through the NIP to the immunocompromised aged 18+ and to the immunocompetent from the age of 50.
5. HAEMOPHILUS INFLUENZAE TYPE B (Hib)
Hib is a very nasty bug that can cause many infections including pneumonia and meningitis. The vaccine often comes as Hib/MenC, which is a combination of Hib and Meningococcal C vaccines.
6. MENINGOCOCCAL C (often combined with HiB)
Meningococcal C vaccine is often combined with the HiB vaccine (HiB/MenC). Vaccines for other strains of meningitis may also be recommended, such as Meningitis B and Meningitis ACWY.
The CDC recommends Hep B vaccination for "most adults” so this is something worth discussing with your haematologist. However, be sure to AVOID the attenuated (live) hepatitis vaccines. Note that testing positive for hepatitis can rule you out of a clinical trial.
OTHER VACCINES
Other “non-live” vaccines might be recommended for travel purposes or in the event of a disease outbreak. In the latter case, specific groups might be deemed at higher risk of infection and therefore eligible for vaccination.
M(ONKEY)POX
In 2022, Monkeypox started to spread more widely.
“While monkeypox is concerning, demands our vigilance, and is dangerous to some in our community based on their increased risk of potential exposure because they work in a lab or medical setting, or their demographic, at this time monkeypox seems to pose a less significant risk to those with CLL/SLL compared to the present COVID-19 pandemic.” (See the CLL Society link in Part 4 for more information.)
There are currently at least two smallpox vaccines that are considered to be effective against monkeypox and more specific vaccines are in development.
ACAM2000™ is a live vaccine and should be avoided by people with CLL and their close contacts.
JYNNEOS® is a modified vaccinia Ankara strain vaccine (MVA-BN) that contains a virus that has been altered so it cannot multiply in the human body and is safe for people with CLL. It is given in 2 doses, at least 28 days apart for people 18 years and over. It is in short supply worldwide.
POLIO
A 2022 outbreak of polio in New York led to an alert about polio vaccines in areas where it is circulating.
Most people are vaccinated against polio as children.
“If you have already been fully vaccinated, you probably do not need a booster at this time. Vaccinated adults who are at increased risk of exposure to poliovirus should talk to their health care provider about whether they may need a booster.” (See the Polio entry in Part 4 for more information)
Note: In some places, a live, oral polio vaccine is still available - avoid it.
To read more about the kind of barriers you might meet trying to get your pneumococcal vaccines in Australia and how to overcome them, visit: healthunlocked.com/cllsuppo...
Q. Can I get PCV20 if I've previously had PCV13 + PPV23?
A. Currently, the US guidelines say you can get PCV20 if you've previously received PPV23 but NOT received PCV13. If you have received PCV13 + PPV23 then you may be considered for another PPV23 vaccine if you are immunocompromised and if at least five years have passed since your last PPV23 vaccine. healthunlocked.com/cllsuppo...
Q. Should I get my flu and COVID-19 (and RSV) vaccines at the same time?
Findings In this cohort study of more than 240 million Medicare beneficiaries 65 years or older with and without underlying medical conditions across 50 US states and the District of Columbia, beneficiaries who received PCV13 had a 6.7% lower risk of pneumonia hospitalization overall, including 5.8% to 7.5% lower risk in adults with underlying medical conditions, compared with beneficiaries who did not receive any pneumococcal vaccines.
Percentages can be deceiving ,what does it mean in absolute numbers? How many out of 100,000 people vaccinated versus unvaccinated where hospitalized with pneumococcal infections?
I agree. There's the base fallacy rate used in arguing against vaccinations for example. That's why I included the reference for the study published in Jama Network for those interested in reading about this.
I have received Evusheld twice now. First time was a month after I had Covid then a follow up 3 months later. Prof Tam in Melbourne was very quick to recommend all his patients had it.
Your Local Epidemiologist, Katelyn Jetelina has provided a Cliff notes update of the outcome from the 13th September ACIP meeting with the CDC, which will influence which COVID-19 boosters will shortly be recommended by the CDC. There was no specific mention in theses notes for the immune compromised, unfortunately:-
Today ACIP—an external advisory committee to CDC—had a much-anticipated meeting with one goal: determine who is eligible for an updated Covid-19 vaccine this fall in the United States.
This goes to the CDC Director for approval. Then, technically, you’ll be able to get a vaccine. However, access may be delayed or challenging, and waiting may make sense for some (more on this later).
After last fall’s updated Covid-19 vaccine, 2 myocarditis cases were verified out of ~650,000 doses. This is a much smaller rate for than the primary series. (We think this is because the increased time interval between doses reduces risk.) However, there is limited data, so this estimate has some uncertainty.
Long Covid remains a risk.
Updated vaccines worked last fall.
Vaccines are cost-effective for those >65 years old.
This is the first time the government is not paying for Covid-19 vaccines. Pfzier/Moderna is charging ~$120-129 per dose and Novavax is ~$130.
Updated vaccine formula remains a good choice.
Pharma companies showed increased antibodies against currently circulating variants, including the newer BA.2.86. (see image)
Addendum: Just prior to the ACIP meeting, the FDA "fully approved the monovalent messenger RNA vaccines (aimed at omicron XBB subvariants of SARS-CoV-2) for people aged 12 years or older and authorized them for emergency use among people aged 6 months to 11 years. The vaccines are now given in one dose instead of two, but the FDA authorized additional doses for certain immunocompromised groups of people.
:
Omicron XBB viruses have emerged to become the predominant SARS-CoV-2 viruses globally and in the U.S. and currently make up all circulating lineages in the U.S.
Moderna and Pfizer-BioNTech in August announced that their updated shots are effective against EG.5 and FL.1.5.1, among other XBB viruses."
Katelyn Jetelina 'Your Local Epidemiologist' has provided "A response to Florida Surgeon General's anti-human remarks" here: open.substack.com/pub/yourl...
She ends with Common ground
It’s important to acknowledge there are points we agree on:
- Medication (i.e., Paxlovid) is an important tool.
- FDA should push for more evidence. This has been a loud theme from VRBPAC—the external committee to the FDA—throughout the pandemic. Why aren’t we getting T cell data? Why aren’t we getting B cell data? Why can’t we find correlates of protection for antibodies? We should demand data from pharma companies.
- We should always work towards better vaccines. Thanks to the $5 billion Operation Next Gen we are developing next-generation vaccines that prevent transmission (like nasal vaccines) or are variant-proof (like pan-coronavirus vaccines).
Bottom line
Framing public health as anti-human is an incredibly dangerous game to play.
Health policy decisions need to be grounded in an accumulation of evidence that provides a comprehensive picture of reality. He combines legitimate points with profoundly foolish ones, which muddles the picture, creates a sense of false equivalency, and makes it difficult for the general public to discern the truth.
Keep this in mind when decision-making about Covid-19 vaccines this fall.
Neil
10.4 to 18.7 fold rise by day 29 for XBB1.5, XBB.1.16, EG.5.1 and BA.2.86
Thanks, Neil. It's an excellent guide and gives a lot of very helpful, reliable information about the vaccines that will be available in the US this Fall and, hopefully, elsewhere before too long.
Katelyn Jetelina 'Your Local Epidemiologist' has provided a subsequent update which answers some FAQs about the next vaccination round including how long to wait after vaccination/infection before getting one of the new vaccines.
lankisterguy recently shared a link to that update in this post:
Also this week, Patient Power featured an article about why CLL patients need to remain vigilant and stay protected with measures that include being up to date with COVID-19 vaccinations.
That article discusses two retrospective cohort studies published online on Aug 31 2023 that "drive home the point that people with cancer, and particularly those with blood cancer, have been at elevated risk . . . These studies, which examined data during previous waves of the pandemic, should encourage continued vigilance among cancer patients as new variants arise, researchers say."
“People with cancer need to know that COVID-19 is not over for them. Unfortunately, it remains a threat to their health and well-being, and this is especially true for people with blood cancer” [Lisa Hicks, MD, MSc, FRCPC]. “Because the world has opened up and masking is much less prevalent, it is more important than ever that people with cancer take actions to protect themselves from COVID-19”
Sequentially for those who remained seronegative after their most recent dose, seroconversion occurred in 40.6% (13/32) after D4, 46.2% (6/13) after D5, 16.7% (1/6) after D6, and none (0/1) after D7 or D8 (supplemental Table 1).
However, importantly, and in contrast to those with no detectable antispike antibody, patients with CLL with detectable but low-level antispike antibodies frequently achieved a higher level of antibody with subsequent doses and the level typically progressively increased with each subsequent vaccine dose (Figure 1A,C). Hence, the ultimate seroconversion rate for CLL was 94.2%, of whom 79.1% achieved antispike antibody levels ≥1000 AU/mL; 54.1%, ≥5000 AU/mL; and 34.1%, ≥10 000 AU/mL. The later and higher antispike antibody levels were commonly associated with neutralization activity against all major COVID-19 variants, including Delta and Omicron.
Early Estimates of Updated 2023–2024 (Monovalent XBB.1.5) COVID-19 Vaccine Effectiveness Against Symptomatic SARS-CoV-2 Infection Attributable to Co-Circulating Omicron Variants Among Immunocompetent Adults — Increasing Community Access to Testing Program, United States, September 2023–January 2024
Receipt of updated COVID-19 vaccine provided approximately 54% increased protection against symptomatic SARS-CoV-2 infection compared with no receipt of updated vaccine. Vaccination provides protection against JN.1 and other circulating lineages.
This post is pinned so it will appear in our list of pinned posts which you can see to the right of your screen (or by scrolling to the bottom of your screen, depending on what type of device you are using) whenever you are viewing any post in our community.
If you also want to save it, you can do that by using the 'save' option immediately underneath the main post. Our pinned post about how to navigate the site gives more detail: healthunlocked.com/cllsuppo...
Thanks so much for writing this post, CLLerinOz . I was struggling to keep up with all the changes recently, and am very grateful to you for taking over the task! I know what a lot of work it involves..
Thanks for all your hard work, not only on the original post, which helped countless people, but also for your support and input into the drafting process for this new post. 😀
Thank you CLLerinOz , Jm954 and PaulaS for this very helpful, comprehensive post!!!
Your list is our list with the added need for us to get a recommendation for how close/far we can spread them apart.
We are aware that several can be given at the same time (ow!), however I believe there are a couple that need to be parsed separately… and, since some may illicit symptom-like discomfort, we want to be sure to allow time for recovery between jabs.
Re: TDap - We we’re told by a pediatrician to make sure that anyone who plans to spend regular time around a baby should also have this one up to date.
When you are in 'catch up' mode after diagnosis and have to get a few vaccines at once, as a general rule, there is usually no reason why more than one vaccine can't be given in the same visit. Technically, there is no limit and only a very small number of vaccines are exceptions to this. The one which is of particular interest to CLL patients relates to pneumococcal vaccination and the scheduling of these vaccines is covered in Part 3 of this post.
If you are getting more than one vaccine in the same site (eg arm), it's recommended that they be separated by at least an inch so any localised reaction is less likely to overlap. Another alternative is to use different sites (eg arms) for each vaccine so, at least, you'll know which vaccine is responsible if you have a localised reaction like swelling. Using two arms is particularly important if you get a pneumococcal vaccine at the same time as the DTP vaccine as each can cause a local reaction.
Where time allows, though, and it's only a case of, say, two vaccines, some people, particularly those who have a history of reacting to vaccines, prefer to split them across separate visits. This enables them to deal with just one vaccine at a time and also has the benefit of allowing them to identify which, if any, vaccine causes them to experience any adverse event.
I just looked back at my own vaccination record and see that I received D/T/P, Hib and Pneumococcal on the same day, and remember both arms were involved. I don't recall any adverse reaction.
I did split my latest flu and Covid-19 vaccinations, even though it was possible to have them together, and this was just a personal preference at the time.
very informative post thank you, my haematologist said getting the new pneumonia vaccine probably wouldn’t work for me, so he didn’t recommend it, also interesting the part about BCG, this is the treatment I was receiving for bladder cancer, but I have had to stop this when starting acalabrutinib and having heart problems, I’m wondering now if it was all linked. Dave
Good morning, wow, I am blown away by your thorough, organized and timely post. What an amazing gift to our community. Thank you for all your hard work to help us stay safe and make good decisions. You are a treasure.
I've updated our main post (above) with an important piece of vaccination information for those who have received (or are about to receive) Chemotherapy treatment for CLL.
Thank you CLLerinOz, for this post - came upon it when searching re live vaccines. I am a nurse and my serology has come back that I've had negative exposure to mumps & rubella. I'm sure I had mumps as a child (I'm now 59), but anyhoo, my new employer wants me to have the MMR vaccine. I had it 11 years ago pre CLL and chemo. As it's a live vaccine should I decline it? I'm trying to research it and finding various confusing answers! I finished FCR Oct 2017 and remain in a stable remission, thankfully, at this stage.Thank you 😊
It's common for healthcare workers to be asked to be vaccinated against certain conditions by their employers and MMR is usually one of those vaccines. However, as you've noted, it is also a vaccine that those with a compromised immune system are advised not to receive as it is a live vaccine.
Although you completed FCR some time ago, your immune system remains compromised and live vaccines are not recommended for you.
It's hard to find a definitive statement in answer to your specific question about how you deal with this in your employment sector. Anything I've seen that is of a more general nature recommends that those who are unable to be vaccinated with MMR on the basis of their compromised immunity and who suspect they have not previously been vaccinated or infected should remain vigilant against infection and seek medical treatment asap should they suspect they have been infected.
You may need something in writing from your CLL specialist to satisfy your employer of your exemption. I see you're in New Zealand. Perhaps someone there will see this who may have advice specific to your location or others may know more about how this requirement is dealt with in your industry elsewhere.
Thank you CLLerinOz for your reply 🙂 The reason I asked you is because I now live in Australia, or paradise, as I call it. 😉Yes, I am well aware of the vaccine requirements in my role and I'm not concerned at all with addressing it with my employer, but thank you for addressing that. I am really unsure whether I should proceed to having a live vaccine, given my post chemo compromised immune system. You have kindly answered that for me and I will now proceed to getting a dispensation from my hematologist in NZ. I feel very fortunate that I'm one of the few people I know who hasn't yet had covid, so hoping my immune system isn't too compromised given that fact!
Three cases of tetanus, including one causing death, have been reported in New South Wales in Australia this year. Although these are the first cases reported there since 2019, NSW Health put out an alert this week to remind people to check that their tetanus vaccination status is up-to-date.
NSW Health, in line with guidelines in the Australian Immunisation Handbook, recommends that:
"A tetanus-containing vaccine booster is recommended for all adults at 50 years of age and at 65 years of age if it is more than 10 years since the last dose.
Vaccination is recommended every 10 years for travellers to countries where health services are difficult to access. Travellers with a higher risk of a tetanus-prone wound are recommended to be vaccinated every 5 years.
Adolescents and adults who have never had a tetanus-containing vaccine are recommended to receive 3 doses of tetanus-containing vaccine with at least 4 weeks between doses, and booster doses at 10 years and 20 years after the primary course."
Very good info. I am meeting next week with my oncologist to discuss when we start my v+o treatment. As Neil has suggested be sure your vac are up to date. I have done that with my Primary care Dr. I am up to date with one possible addition. I have had Prevnar13 and 23. Prevar 20 is not live but I haven't found if you should take before starting treatment. CDC recommends talking to your Dr. My primary suggests I should get it. I'll talk to my oncologist this week . Are you aware of any specific info regarding this vac and CLL. Thanks
Well done for getting up-to-date with your vaccinations before starting your venetoclax + obinutuzumab treatment.
In its article about vaccinations for people with CLL, the CLL Society says this about someone in your situation:
“CLL/SLL patients who previously received a dose of PCV13 should have a PPSV23 at least eight weeks later. If you were younger than 65 when the first dose of PPSV23 was given and have not turned 65 years old yet, you should receive a second dose of PPSV23 at least 5 years after the first dose of PPSV23. This is the last dose of PPSV23 that you should be given before 65 years of age. Once you turn 65 and at least 5 years have passed since PPSV23 was last given, you should receive a final dose of PPSV23 to complete all pneumococcal vaccinations. At this time, additional pneumococcal vaccines are not being recommended by the CDC.”
You can read the full article, including information about Prevnar 20, here:
Interesting - I was approved to take the live oral cholera vaccine after completion of my CLL treatment for travel to Lebanon during the outbreak there last year.
There are two main types of cholera vaccines and different countries approve different types and brands. In 2021, a report found that cholera vaccination recommendations in Europe "vary considerably between countries" pubmed.ncbi.nlm.nih.gov/333...
One type of cholera vaccine consists of live attenuated bacteria and this type of vaccine is not usually recommended for people who are immunocompromised.
In a previous discussion you explained that your doctor checked your immunoglobulin levels before deciding to proceed with giving you the live vaccine. Other factors may have included the time you had available. The live vaccine is only one dose which needs to be taken at least 10 days before travel. The non-live vaccine involves two doses that have to be taken 7 to 14 days apart. In addition, your body would usually take a couple of weeks after vaccination to develop protection against diarrhoea due to cholera.
Vaccination should be seen as a complement to other disease prevention measures. As far as efficacy is concerned, in tests with healthy participants, the live vaccine "was shown to be 90.3% effective against V. cholerae 10 days after vaccination and 79.5% effective 90 days after vaccination." ncbi.nlm.nih.gov/pmc/articl...
For the non-live vaccine, "Most people will produce enough antibodies to protect against diarrhoea due to cholera. However, as with all vaccines, 100% protection cannot be guaranteed. About 85% of people can expect to be protected against cholera in the 6 months following initial vaccination. This decreases to 52% at the end of the second year, when a booster should be given." nps.org.au/assets/medicines...
For the benefit of others reading this, I'll give a bit more detail about the two main vaccines that are used in travellers to help protect against cholera:
1. Live Vaccine- its safety and efficacy has not been tested in people who are immunocompromised
Vaxchora™ is a live vaccine, used mostly in the US in people aged 2-64 and in the EU in those aged >2 who are travelling to an area of active cholera transmission.
The FDA package insert for Vaxchora™ states: "The safety and effectiveness of VAXCHORA have not been established in immunocompromised persons. The immunologic response to VAXCHORA may be diminished in immunocompromised individuals. VAXCHORA may be shed in the stool of recipients for at least 7 days. There is a potential for transmission of the vaccine strain to non-vaccinated close contacts (e.g., household contacts). Use caution when considering whether to administer VAXCHORA to individuals with immunocompromised close contacts." fda.gov/media/128415/download
The European Medicines Agency states that "People who were born with problems with their immune system or are receiving treatment that weakens the immune system must not take Vaxchora." ema.europa.eu/en/medicines/...
As a live attenuated vaccine, concomitant administration of Vaxchora™ with systemic antibiotics is not recommended since these compounds may be active against the vaccine strain. Hence it is not recommended to administer Vaxchora™ to patients who have received oral or parenteral antibiotics within 14 days prior to vaccination. This may also limit the utility of Vaxchora™ in outbreaks where the use of antibiotics may be an important part of the outbreak response." ncbi.nlm.nih.gov/pmc/articl...
2. Inactivated, Non-live Vaccine - people who are immunocompromised can receive this vaccine
Dukoral™ is a non-live vaccine that is "authorized in Europe, Australia, Canada, Switzerland, New Zealand, Thailand, and the United Kingdom" but is not available in the US. It is most commonly given to travellers "whose activities or medical history put them at increased risk, including:
- aid workers
- people going to areas with cholera outbreaks who have limited access to safe water and medical care
- those for whom vaccination is considered potentially beneficial (people who do not fit into the above groups, but are still considered at higher risk)." mail.travelhealthpro.org.uk...
Dukoral™ consists of 4 different inactivated strains (types) of V. cholerae serotype O1, and a "purified recombinant DNA-derived B-subunit of the cholera toxin". People who are immunocompromised can receive it but the vaccine may provide a lower level of protection than it does for people with healthy immune systems. precisionvaccinations.com/v...
In 2022, it was reported that the world was experiencing the highest number of cholera outbreaks in recorded history at the same time as a shortage of cholera vaccines. The following article that appeared in Deutsche Welle in April 2022 explains more about that: dw.com/en/why-is-the-world-...
Thank you for the reminder and the extra info - this is more than what my doctors explained and incredibly helpful for assessing the situation next time!
To make a decision about RSV vaccination, the CDC recommends using shared decision-making (SCDM), which means that health care providers should talk to eligible individuals about whether RSV vaccination is appropriate for them. cdc.gov/vaccines/vpd/rsv/hc...
The above link also answers other frequently asked questions about RSV vaccination.
Until studies are available for the immune compromised, it's possible there will be some variance in the position taken by CLL specialists. healthunlocked.com/cllsuppo...
In a notice sent to clinicians on September 05, 2023, the CDC noted "increases in respiratory syncytial virus (RSV) activity across some parts of the Southeastern United States in recent weeks . . . Historically, such regional increases have predicted the beginning of RSV season nationally, with increased RSV activity spreading north and west over the following 2–3 months."
In that statement, the CDC recommended that:
"Vaccination should be prioritized in adults ages 60 years and older who are most likely to benefit, including those with certain chronic medical conditions associated with increased risk of severe RSV disease, such as heart disease (e.g., heart failure, coronary artery disease), lung disease (e.g., chronic obstructive pulmonary disease [COPD], asthma), and immunocompromising conditions. Adults with advanced age and those living in nursing homes or other long-term care facilities are also at increased risk of severe RSV disease and may benefit from RSV vaccination." (my emphasis) emergency.cdc.gov/han/2023/...
Efficacy of the new vaccines has been measured at 82-86% but, as with all vaccines, those who are immune compromised may not achieve this result.
RSV vaccines are expected to be more durable than flu vaccines and should offer protection in those who are not immune compromised throughout the RSV season and perhaps for the following year's season, too. To date, I'm not aware of any studies that show how durable the vaccines might be for the immune compromised although it will possibly be shorter.
Other posts with more detailed information about RSV vaccination include:
I had even more meningitis vaccinations than that. The one they normally give teenagers. And I got RSV privately since I am in the UK and it is not yet available on the NHS.
It's good that those who can afford it can at least access the RSV vaccine privately in the UK.
I'm wondering if you might have been considered more at risk for your meningococcal vaccinations due to personal circumstances or because of where you live or travel intentions. In Australia, CLL isn't routinely included in the list of specified medical conditions associated with increased risk of invasive meningococcal disease.
Interesting. I live in inner London and at the time was parent to a teenage child. The local hospital is supervising me. I got a meningitis vaccination that they are giving all teenagers.
Londoners may be interested in the fact I used a pharmacy in Hampstead to get the RSV vaccination and it cost me £230.
For those in the US, this is a reminder that the 2024 vaccination schedule that was released in November 2023 is now available and effective.
The main changes since the previous schedule was released that are relevant for those with CLL are the addition of new vaccines for respiratory syncytial virus (RSV), released in the Fall 2023, and the 2023-2024 formulation of the updated COVID vaccine (both mRNA and protein-based adjuvanted versions).
It also provides comprehensive advice about pneumococcal vaccination by providing recommendations based on any vaccination someone might have already received.
The general schedule now also includes the mpox vaccine (Jynneos) and a new MenACWY-MenB combo vaccine with notes relating to the use of these vaccines in particular populations.
With respect to the risk from respiratory infections for which we have vaccinations, the USA's CDC maintains a RESP-NET interactive dashboard cdc.gov/surveillance/resp-n...
"Surveillance is conducted through a network of acute care hospitals in select counties or county equivalents in 12 states for RSV surveillance, 13 states for COVID-19 surveillance, and 14 states for influenza surveillance. The surveillance platforms for COVID-19, RSV, and influenza (known as COVID-NET, RSV-NET, and FluSurv-NET, respectively) cover more than 30 million people and include an estimated 8-10% of the U.S. population."
Caitlin Rivers maintains a "Force of Infection" Substack report to which you can subscribe. It too covers the above respiratory infections, plus she also covers stomach bugs and food recalls. Here's her US National Outlook report to the 15th February.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")