We've had a couple of members mention that they are positive for SF3B1 Mutations so I thought it would be worth a short simplified post about it.
SF3B1 are predominantly sub clonal genetic events in CLL and are not unique to CLL as they are also found in other haematological disease such as myelodysplastic syndrome. The frequency ranges from 5% to 18% of patients, depending on the various cohorts of patients depending on the proportion of cases 1) at presentation, 2) at the time of treatment or 3) at disease progression. Even 1.5% of individuals with the CLL precursor condition, monoclonal B-cell lymphocytosis (MBL) will have the SF3B1 mutation.
As it’s a sub clonal mutation, not all the CLL cells are affected and it will have evolved after the development of CLL. Although the link between the SF3B1 mutation and CLL pathogenesis (progression) is unclear, some evidence suggests that the SF3B1 mutation might be associated with less genomic stability and epigenetic modification and therefore a more aggressive and unpredictable disease.
Recent studies have provided a consistent picture that the SF3B1 mutation is associated with more aggressive disease and poorer clinical outcome. There is a strong association with the 11q del subtype of CLL which also shares the same prognostic features.
A study of Scandinavian patients identified only 3.6% with mutated SF3B1. However, statistically those patients had a significantly worse overall survival and earlier time to treatment.
Another large study of 1124 newly diagnosed CLL patients from the German CLL Study Group (GCLLSG) confirmed that SF3B1 mutations are associated with a shorter time to first therapy and with unmutated IGHV status. Both of those characteristics are also common features of 11q del CLL and a less favourable prognosis than other mutations.
500 cases from a prospective and controlled clinical trial (the UK LRF CLL4 trial) demonstrated a high rate of SF3B1 mutation (17%) in patients requiring immediate treatment i.e with no watch and wait. Again, the presence of mutation was associated with significantly worse overall survival and with a trend toward shorter progression-free survival.
However, and this is a big point. I can’t find anything very recent that addresses the survival of SF3B1 patients in the era of novel agents. The vast majority of 11qdel and unmutated patients, with and without SF3B1, do very well on target treatments and, at the moment, there is no evidence that the SF3B1 patients do worse than 11qdel and unmutated without SF3B1.
On a positive note SF3B1 mutation does not confer the same degree of poor prognosis as TP53 mutation or 17p deletion.
If and when these patients need treatment they should have a targeted therapy or look for a clinical trial of novel agents, rather than have chemo-immunotherapy such as FCR, BR or Chlorambucil.
Jackie, I had a Molecular Diagnostic testing at MDA that showed SF3B1 and Notch1 mutations at various locations, but the VAFs, which I assume means frequencys, were below 5 or 10%. Are you aware of any cut off point in frequency where these mutations are considered to be irrelevant?
This paper is complicated but this paragraph sums up the significance of the burden of mutations such as SF3B1 and NOTCH1. They used an ultra-deep-NGS strategy with a bioinformatic algorithm for the highly sensitive detection of small mutated subclones in the NOTCH1, SF3B1, and BIRC3 genes.
'There was no statistically significant difference in OS between patients harboring small subclonal mutations of NOTCH1, SF3B1, or BIRC3 and wild-type patients (non mutated) (Figure 2A–C), even after adjusting for confounding factors (Online Supplementary Table S6). The study, however, was not fully powered to support non-inferiority.
Conversely, patients harboring small subclonal mutations of NOTCH1, SF3B1, or BIRC3 showed a trend towards a longer OS than patients having a mutation that was detectable by Sanger sequencing (Figure 2A–C). Consistently, outcome-driven approaches documented that NOTCH1, SF3B1, and BIRC3 mutations should be represented in at least 25%, 35% and 1% of the alleles, respectively, to have the maximum impact on CLL OS (Online Supplementary Figure S3). Application of these approaches to TP53 mutations failed to identify a clear cut off, suggesting that, in contrast to NOTCH1, SF3B1, and BIRC3 mutations, TP53 lesions are relevant to the outcome of CLL independent of their abundance.'
and then repeated later in the paper - 'The clinical impact of small subclones harboring NOTCH1, SF3B1, or BIRC3 mutations appears to be less pronounced than that of small TP53 mutated subclones. Also, upon treatment, NOTCH1, SF3B1, and BIRC3 mutations to do not provide small subclones with the same strength of fitness advantage as TP53 mutations.'
The paper is here: Clinical impact of small subclones harboring NOTCH1, SF3B1 or BIRC3 mutations in chronic lymphocytic leukemia - ncbi.nlm.nih.gov/pmc/articl...
It sounds as though your 5-10% may not be significant.
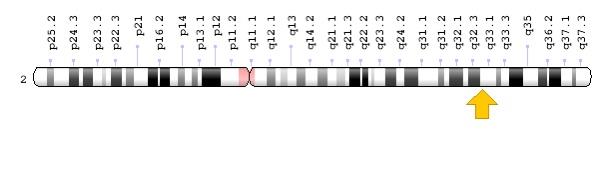
Jackie, this is where I get confused. Is not sf3b1 located on the second chromosome?
I would think based on the correlation between 11q Cll and sf3b1 mutations that the sf3b1 gene would be located on the q arm of the 11th chromosome next to the ATM gene. But when I looked it up earlier this year I saw something saying it’s on the second chromosome. Maybe I am looking at the wrong gene.
And if sf3b1 is on chromosome 2, how does it correlate to 11q Cll?
My understanding today of how genes work is light years ahead of where it was three years ago. That said, if you had a knowledge scale for genes and how they work of 1 to 100, with 1 being ignorant and 100 being a molecular biologist, I would be somewhere in the 5 range, a tad above ignorant. It’s way over my head. But I do enjoy learning about it.
I didn't mention that but yes, SF3B1 (Splicing Factor 3b subunit 1) is located on chromosome 2. I think we have to accept that there is a strong association with 11q del and unmutated IGHV but causation and dependancies are unknown at the moment.
There's a lot we don't know but these deep sequencing studies might throw more light on aetiology - eventually!
Thanks Jackie for another informative post! It's so helpful to have someone with your background to provide this type of information on the forum so it can be discussed and further our frame of reference.
So much better than Dr. Google. Thank you for all your efforts - it makes such a difference!
Thank you for your post, being one of those with the SF3B1 mutation it is interesting, are there differences as in hotspots or not etc? Mine was on a hotspot location and not only confined to cll but in other locations I think I may have mentioned in previous posts.
Thank you Jackie. So useful to have someone with your technical experience to share with us, and for all the extra work you do behind the scenes with drug approvals.
Jackie, thanks for this excellent article. Couple of questions for you which may not be answerable
Do you know whether this SF3B1 mutation is like IGHV unmutated status whereby at least some people can do well on chemo as so far I seem to have personally ? Or is it more analogous to 17p/TP53 where Chemo is basically not helpful at all?
I know you work on access to medicines in the UK, and of course at the moment only two markers are sufficiently recognised by NICE to allow us to skip chemo and move straight to targeted treatments. (17pdel and TP53 for any readers unaware of which they are).
Will there be any moves from the CLL Support charity to try to appeal to NHS in some forum to consider adding other mutations / deletions to the rather short list of chemo skipping?
I note for example that NHS England did make some formal changes changes to chemo vs selective drugs during the pandemic. Despite some comments from cll specialists and some evidence of some people being able to get Acalabrutinib unfortunately CLL was not formally on this list which of it was would give patients an option to avoid chemo at least during covid (which sounds like it’s here for a while). Can something be done here? Should there be some kind of campaign like previously? See england.nhs.uk/2020/08/covi...
It can cause a lot of anxiety among our UK members and those from many other countries to hear they have markers that suggest chemo should not be given but they have to have it anyway. I remember that anxiety only too well personally.
You're right, I can't answer your first couple of questions! There simply isn't the data and even more difficult is that SF3B1 is not routinely tested for (or even in a trial/research setting?) so the information is even more elusive.
Given the association with NOTCH1, I would be more interested to know if the SF3B1 mutation is associated with a higher or earlier incidence of Richter's transformation. Again, the level of burden of mutation is important as in the second reference I quoted. The only exception I know of is TP53 where any level of mutation is going to adversely affect PFS after treatment. Apologies for referring to one of my own posts but this one 9 months ago discusses TP53 in more detail. healthunlocked.com/cllsuppo...
Regarding your point about non chemotherapy treatment and NICE/NHS England - during the pandemic lockdown all CLL patients who needed treatment and could not wait had free access to Acalabrutinib and the UK CLL Forum circulated information (reported on this forum) giving the details of how to access it. No patient should have had to have chemo during this time.
However, I know the access was being reviewed at the end of July and I don't know what the outcome was and if there is still any access to Acalabrutinib.
The unmutated IGHV group are a huge concern as they do not do well with chemotherapy. FCR as a first therapy produces a median PFS of 55 to 57 months across all subtypes but this is heavily skewed by the unmutated patients. In addition, it's well known that FCR-related AEs can be severe and long lasting leading to further ill health and mortality.
The median for progression free survival of the unmutated group is only approximately 3.5 years or 40 months so the charity is working hard to get access to targeted treatments for this group. Those FCR related adverse event also impact more heavily on the public purse and this is just one of the rationale we have been using for change.
I'm bound by a confidentially agreement with NICE so I cannot report on any recent developments but any changes will be reported here as soon as I am able to do it.
Hope this gives you some answers that you were looking for.
Thanks Jackie. And thanks for what you are doing behind the scenes. It’s odd that the Acalabrutinib thing was never actually formally listed by NHSE as one of their covid changes on the page I shared in my last comment. And some members were not always able to get access to it. Particularly some non expert sites seemed to be totally unaware of the idea.
I think we got to the bottom of it as there was a special patient access program from the company but only for patients who were “contraindicated for chemo”.
So some specialists argued, I believe correctly, that FCR was contradictated for everyone during the pandemic. Not sure if that argument is still being accepted right now.
But I do note that there is an Acalabrutinib safety study that is not yet open but coming soon only in ten sites. (Will list them at the end).
One thing that’s worth pointing out for those who’ve been forced like me to get FCR despite being unmutated is that there are a subgroup of us who do Quite well on FCR. If you get to MRDU status as I did (and at less than 1 in 100,000) then ⅔ of patients will get at least five years before needing another treatment. So far I am approaching 2 year since starting treatment and still have a lymphocyte count of less than one.
So whilst I absolutely back your efforts to extend access and would be happy to share testimony of what being treated with FCR is like if that would help, I think it’s important to note some of us do well.
And of course fortunately here in the UK we can now get second line teatment with either V plus R or I freely. Which should hopefully avoid most of the bad outcomes seen in some of the trials where due to the time they were done few people who relapsed were able to get access to selective treatments.
And so it would be great if it also became easier to access IVIG which in my view is shamefully being rationed and many more of us would likely benefit from this especially as anti covid antibodies continue to rise in the preparations. It is surly time for the UK to have a major drive to collect more plasma and make IVIG ourselves again.
I think we would lose less people to infections if we were less restrictive with the IVIG and also If offering prophylaxis and immunisations were more consistent.
infecfion management is also where a 24/7 nurse led helpline can be very helpful and I would like to see that kind of service which only a few hospitals havd rolled our nationwide.
Every CLL patient could be assigned to a specialist centre that runs such a helpline even if they had their regular appointments more locally and the nurses can and do also call up local A and E departments to tell them their patients are coming in and what protocol needs to be followed.
Alongside this theee is a major need for formal guidelines for GPs and A and E on issues like being more ready to treat wirh antibiotics and for longer courses, that people can be sicker than they look due to sluggish immune systems, and when to offer prophylaxis and immunisations and which ones. This could be a nice project to draw the experts together for.
It does seem to me that if we are going to spend loads of money treating people with wonderful new drugs the system needs to do a much better job of managing the infection risk that all current treatments do sadly increase (some more than others)
Anyway I digress. Sorry for drifting off topic there.
But here’s the list of the Acalabrutinib study sites (this is differnt to the study in Canterbury ) see clinicaltrials.gov/ct2/show...
Adrian, I'm sorry to contradict you but your sentence "I think we got to the bottom of it as there was a special patient access program from the company but only for patients who were “contraindicated for chemo” is incorrect.
The objective was/is to keep people away from hospitals and iv treatment or any treatment that needed a lot of hospital supervision or intervention eg Venetoclax. Chemo was effectively contraindicated for everyone during the height of the pandemic lockdown.
Any patient that needed treatment and could not wait should have been able to access the scheme via their doctor. The contact email at Astra Zeneca was included in the details issued by the UK CLL Forum guidance.
That guidance has now been reissued and amended for the Post Lockdown period and patients can still access Acalabrutinib provided they meet the inclusion criteria for the Elevate Trial (TN) which are pretty wide. I'll post on this separately to keep everyone updated.
Someone’s consultant told them they couldn’t qualify for the program as FCR was not specifically contradicted
They shared the specifics of the company program and it definitely matches what I said. I looked at it again this morning.
Turns out however that it wasn’t shared in here but on the young Person WhatsApp group thats run by two of the CLL support trustees. It is a PDF. Here is the exact wording.
———-
_________
_________
Patient access to Acalabrutinib for first-line treatment of chronic lymphocytic leukaemia (CLL) prior to EU licence and NICE reimbursement.
This letter is a reply to your enquiry about possible access to acalabrutinib before EU licence is granted for adult patients with previously untreated CLL who are ->-65 years of age, or < 65 years of age who are FCR (Fludarabine, cyclophosphamide, rituximab) ineligible, in the 1st line(1L) setting.
The acalabrutinib IL CLL Early Access Programme
AstraZeneca has set up an Early Access Programme (EAP) to provide free access to acalabrutinib for eligible patients following the results from the ELEVATE-TN clinical study. In the ELEVATE-TN study acalabrutinib in combination with obinutuzumab, acalabrutinib monotherapy, and obinutuzumab plus chlorambucil were evaluated in a randomised, multicentre, open-label, actively controlled trial in 526 patients with previously untreated CLL, published in the Blood (2019) 134 (Supplement_l):
The acalabrutinib EAP will be for patients eligible for acalabrutinib in monotherapy or in combination with obinutuzumab for previously untreated CLL, adult patients who are 65 years of age, or < 65 years of age *******who are FCR-ineligible******, in the 1st line setting consistent with the ELEVATE-TN entry criteria (Please see below for full inclusion and exclusion criteria).
Acalabrutinib is currently not licensed for patients in the UK and El-J. The recommended dose of acalabrutinib monotherapy is 100 mg taken orally approximately every 12 hours until disease progression or unacceptable toxicity.
The recommended dose of acalabrutinib in combination with obinutuzumab is 100 mg taken orally approximately every 12 hours until disease progression or unacceptable toxicity. Starting acalabrutinib at Cycle 1 (each cycle is 28 days). Start obinutuzumab at Cycle 2 for a total of 6 cycles and refer to the obinutuzumab prescribing information for recommended dosing.
Administer acalabrutinib prior to obinutuzumab when given on the same day. Please note
AstraZeneca will not supplv obinutuzumab for eligible patients. AstraZeneca will only supplv acalabrutinib for eligible patients.
Please refer to the inclusion / exclusion criteria below to check for initial patient eligibility for this early access programme ahead of your submission request:
INCLUSION:
Job bag no: GB-21020 Date of prep: March 2020
1. Patient has untreated CLL and is either:
a. 2 65 years of age, OR
b. >18 and <65 years of age provided that at least one of the following criteria is met:
i. Creatinine clearance 30 to 69 mL/min using the Cockcroft-Gault equation ii. A
score higher than 6 on the Cumulative Illness Rating Scale-Geriatric (CIRS-G)
2.Diagnosis of CD20+ CLL that meets published diagnostic criteria (Hallek et al
2008 https:/(doi.org/10.1182/blood-2007-06-093906) as listed below:
a.Monoclonal B cells (either kappa or lambda light chain restricted) that are clonally co-
expressing 1 B-cell marker (CD19, CD20, or CD23) and CD5
b. Prolymphocytes may comprise 55% of blood lymphocytes
c. Presence of 5 x 109 B lymphocytes/L (5000/gL) in the peripheral blood (at any point since
diagnosis)
3. Active disease meeting 2 1 of the following IWCLL 2008 criteria for requiring treatment
EXCLUSION:
1. Any previous systemic treatment for CLL (note: Prior localised radiotherapy is allowed).
2. Potential eligibility to participate in an ongoing clinical trial sponsored by AstraZeneca/Acerta for the same indication as this EAP in the UK (Patient eligibility to participate in an ongoing clinical trial will be checked by AZ UK).
3. Knowncentralnervoussystemlymphomaorleukaemia.
4.Known prolymphocytic leukaemia or history of, or currently suspected, Richter's syndrome.
5. Confirmed 17p del and/or TP53 mutations, with eligibility for currently reimbursed novel
inhibitor treatment ibrutinib, idelalisib + rituximab or venetoclax in the NHS
6. Uncontrolled autoimmune haemolytic anaemia (AIHA) or idiopathic thrombocytopenic purpura (ITP), defined as declining haemoglobin or platelet count secondary to autoimmune destruction currently or requirement for high doses of steroids (> 20 mg dose of prednisone
for other medical conditions such as inhaled steroid for asthma, topical steroid use, or as premedication for administration of acalabrutinib or contrast. For example, patients requiring steroids at daily doses > 20mg prednisone equivalent systemic exposure daily, or those who are administered steroids for leukaemia control or white blood cell count (WBC) lowering.
a)Malignancy treated with curative intent and with no evidence of active disease present for more than 3-years before EAP application date and felt to be at low risk for recurrence by treating physician.
b) Adequately treated lentigo malignant melanoma without current evidence of disease or adequately controlled non-melanomatous skin cancer.
c)Adequately treated cervical carcinoma in situ without current evidence of disease.
10.Significant cardiovascular disease such as uncontrolled or symptomatic arrhythmias, congestive heart failure, or myocardial infarction within 6 months of this application, or any Class 3 or 4 cardiac disease as defined by the New York Heart Association Functional Classification, or QTc > 480msec.
11.Unable to swallow capsules or malabsorption syndrome, disease significantly affecting gastrointestinal function, or resection of the stomach or small bowel or gastric bypass, symptomatic inflammatory bowel disease, or partial or complete bowel obstruction.
12.Uncontrolled active systemic fungal, bacterial, viral, or other infection (defined as exhibiting ongoing signs/symptoms related to the infection and without improvement, despite appropriate antibiotics or other treatment) or ongoing intravenous anti-infective treatment.
13.Known history of infection with human immunodeficiency virus (HIV).
Job bag no: GB-21020 Date of prep: March 2020
Page 2
14.Planned vaccination with live, attenuated vaccines within 4 weeks of first dose of acalabrutinib.
15.Serologic status reflecting active hepatitis B or C infection. Patients with hepatitis B core antibody positive who are surface antigen negative or who are hepatitis C antibody positive will need to have a negative polymerase chain reaction (PCR) result before access is provided. Patients who are hepatitis B surface antigen positive or hepatitis B PCR positive and those who are hepatitis C PCR positive cannot be provided access.
16.History of stroke or intracranial haemorrhage within 6-months of this EAP application. 17.History of a bleeding diathesis (e.g., haemophilia, von Willebrand disease).
18.Requires or receiving anticoagulation with warfarin or equivalent vitamin K antagonists (e.g.,
phenprocoumon) within 7days of first dose of acalabrutinib.
19.Requires treatment with proton-pump inhibitors (e.g., omeprazole, esomeprazole,
lansoprazole, dexlansoprazole, rabeprazole, or pantoprazole).
20.Breast feeding or pregnant.
21.Current life-threatening illness, medical conditions, or organ system dysfunction which, in
your opinion, could compromise the patient's safety.
22. Concurrent participation in another therapeutic clinical trial.
23.Requires treatment with a strong cytochrome P450 3A (CYP3A) inhibitor/inducer. 24.Presence of a gastrointestinal ulcer diagnosed by endoscopy within 3-months of early access
What happens to the current EAP if acalabrutinib is granted marketing authorisation by the regulatory authorities for treatment in first-line CLL?
AstraZeneca has applied for an EU licence in these patients and this could be granted during the latter half of 2020. This EAP will be open for new requests until 1st April 2021 or reimbursement, whichever is earlier. However, AZ reserves the right to close this EAP for any new patients without notice. Should early closure of this EAP occur, existing patients will continue to be supplied with acalabrutinib for their entire treatment period as long as they
continue to derive clinical benefit with no evidence of disease progression.
In the event of AstraZeneca not being granted a market authorisation for acalabrutinib in the EU, we will continue to supply this at no cost to patients already on the EAP scheme, if they continue to derive clinical benefit (with no evidence of disease progression) as determined by their physician. No new patients will be eligible to enter this EAP in the event of AstraZeneca not being granted a market authorisation for acalabrutinib in the EU.
What happens after a decision on NHS reimbursement?
AstraZeneca will begin reimbursement discussions with NICE before the grant of a marketing authorisation with the aim of securing reimbursement for acalabrutinib in previously untreated CLL in the NHS.
Should acalabrutinib in previously untreated CLL obtain approval for reimbursement within the NHS, AstraZeneca expects as part of the agreement, that you will start immediate and timely transition of your patient(s) from the EAP to NHS prescriptions and commercial
supplies, in line with the reimbursement criteria.
In the event that acalabrutinib does not obtain NICE approval for reimbursement within the NHS, AstraZeneca will continue to provide acalabrutinib at no cost for existing patients who have already started their treatment in the EAP scheme, provided that they continue to derive clinical benefit with no evidence of disease progression.
In the unforeseen situation of NICE approval but lack of NHS authorisation to allow transfer of existing scheme patients onto NHS reimbursed stock, AstraZeneca will continue to supply acalabrutinib at no cost to patients already enrolled onto in the EAP scheme, provided that they continue to derive clinical benefit with no evidence of disease progression.
Next steps
AstraZeneca has appointed Clinigen Group to manage the administration and supply of the acalabrutinib EAP. All decisions related to patient eligibility will be made by the AstraZeneca Medical Team.
To proceed, please contact Clinigen who can provide further information and guide you through the EAP application process.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.