Amazing! The headline states that there is ‘low’ mortality regardless of treatment for local PCa…really? Well, that did not make me feel very good as I opted for treatment! RP, followed by ADT for 6 months, followed by IMRT sRT, followed by 15 months of ADT post treatment…I was not feeling so good about my decision. Then I read the article…this jumps out!
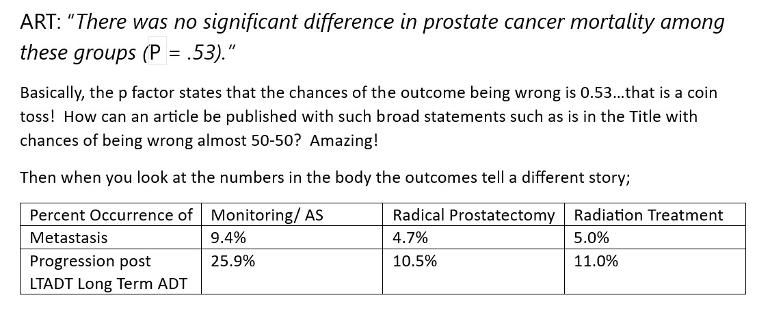
ART: “There was no significant difference in prostate cancer mortality among these groups (P = .53).”
Basically, the 'p factor' states that the chances of the outcome being wrong is 0.53…that is a coin toss! How can an article be published with such broad statements such as is in the Title with chances of being wrong almost 50-50? Amazing!
Then when you look at the numbers in the body the outcomes tell a different story; see the attached image. Yes, the relative risks are low for sure, MET only happens in 9.4% of men on AS (Active Surveillance - monitoring), but that is opposed to 4.7% for RP and 5.0% for RT (4.9% average)…got my calculator out and the risk of having MET while on AS is a whopping 94% higher (double)! Then, ADT treatment for AS to prevent local progression did not do any better. 25.9% of AS with ADT had local progression! That is compared to an average of 10.75% for men who had RP or RT. This means if you choose AS, even if you get ADT, your chances of local progression are 141% higher! Even if I disregard the entry statement, that the reported results are as good as a coin toss, why would I opt to do nothing if I have localized PCa? Its baffling…
There seems to be a strong undercurrent in the treatment community that doing anything that harms anyone is worst than doing something that helps someone avoid a worse outcome. I have my share of ‘do overs’ that I wish I did not do, that perhaps could have been relegated to AS…but, it’s the unknown-unknown we are dealing with. What would have happened had I done nothing, had I waited for sRT and not moved with IMRT at a PSA of 0.13? Had I not done an additional 15 months of ADT after sRT and waited to see if my PSA would start to rise?
Don’t know, but will soon find out…I stopped my ADT December, 2022 and am now post 6 months vacation! So far, so good. Will let you all know how this grand experiment goes. But articles like this bother me. They are not statistically sound and their claims are bold! Be forewarned, PCa treatment is a pipeline with ‘Check Valves’ along the way. You can go forward, but you cant back up…what’s done is done so making decisions based on articles like this is…a coin toss! Heck of a way to treat any disease. Rick
PS the CDC just pulled the Johnson and Johnson COVID vaccine off the market. Why? Side effects such as blood clots, heart damage, etc…AND what was the occurrence of these serious effects? 4-10 in 1,000,000 doses (that is 0.0009%)…read that a couple of times…4 to 10 patients out of a million were affected…and for that a vaccine was pulled and God knows what will happen next to these patients or to J&J…but for PCa we have a study that proports NOTHING be done when single and double digit percentages of men are impacted by MET or local progression, by doing NOTHING…again, amazing.
I too would have done things differently 16 years ago. Its always 20/20 looking backwards. Still glad to be doing BAT at this point. Chemo naive but did about everything else. Let the dance continue.
I read your bio. Very interesting that you are on BAT. If my PSA comes back I will be looking at that treatment. You did not list your high TET levels while on treatment. Can you clarify.
…also look at the post that I have for the various articles that I publish. There’s a lot there on testosterone replacement therapy for prostate cancer patients. If you’re interested and haven’t seen those studies or podcast take a look. If you can’t find them, let me know when I can send them.
Good luck. It looks like you and I are not two that would roll the dice on a 50-50 study that says doing nothing is the same as doing something. I thought it was a cookie title, and despite the P factor that was used to prove conclusion its contents doesn’t support its findings. Amazing.
I think you learn a lot about prostate cancer as you attempt to educate yourself about your disease.
1. There is not cook book treatment much as insurance would like to believe that. This disease is many diseases. Just read the profiles of member of this forum or talk to the people in the waiting are while you are getting RT or sitting in the chemo chair to realize this.
2. When you sort through the numbers there really is not much difference in outcome i.e. death than with breast cancer. The big difference is prostate cancer has been sold as a "benign" old man disease that you can live with until you die of something else; while breast cancer is a young women's disease. Both are horrible and should be looked at as such.
3. Because of the public perception/brainwashing funding for prostate cancer has always lagged more than is should based on the shear numbers of victims of this cancer.
Bottom line IMO is this is not a trivial cancer and should not be looked at as such. It needs more research funding. And importantly, we each need to be treated individually using all the information available, not as single disease entity.
…no my case was possibly different than yours. My decipher score was a staggering, 0.97 out of 1.0. I had a lethal cancer cell type. My extra prostatic extension was negative at the margin, but the surgical biopsy reported pattern 4 or 5 noted. Because of those two things I could not screw around and gamble and allow the cells to escape the fossa area. I think I made the right choice because I took six months of ADT followed by salvage radiation (sRT). At the end of that treatment I had a four month vacation. My testosterone roared back to 278, but my PSA stayed at also uPSA ultra low levels. So if there was any cancer. Causing the .13 it was localize, and it was not metastatic. What I don’t know at this point is if Selles escaped and years later they will show up. But I think I bought myself some time. Here are a couple of good podcasts and so is radiation. Note that the one thing I did deliberately was going to salvage with a low level of leakage. I knew that I would be stuck with this for life, but decided to do it anyway. Again, I made a decision that I could not take any chances. Your situation may be completely different.
What I do regret about not having acted on when I decided to proceed with salvage radiation was a penile implant. I was still under the delusion that I had to wait two years or more to determine if my natural erections would return. I should’ve had. Medical counseling to the contrary. With only half my nerve spared, salvage radiation. And 21 months of ADT treatment my natural erections were never going to come back. Someone should’ve sent me down and told me this. Or at least warn me so that I could make an informed decision. What I suffered was atrophy of my penis. Additional damage from Perroni’s, which started to appear soon after the surgery. That I would do different. Here is my. coulda-woulda-shoulda list of regrets and opportunities. Missed regarding my decision to proceed with the penile implant.
…but one thing remains true to this day. And it’s some thing that I have talked about in these posts. I do think that it’s important to not be too hard on yourself. I think in all instances I acted late, but not too late. I think that in the end, that is the best that we can do given the fact our medical community treats symptoms. No one pays them to take the risk that is required for actions that will prevent outcomes. There are probably too many horror stories told in medical school on what can happen. That is why the patient is ultimately responsible to push the doctor and the medical community in the direction that he ultimately decides is in his best interest. The doctor will always play it safe. You can’t blame them. Here’s what I wrote about my implant. I am now six months post surgery and it’s the best decision that I’ve made so far. I only wish I had done it sooner; it makes me feel whole.
…watch your PSA doubling time. If you don’t have genomics testing, get some to find out what cell type you have. If it’s not an aggressive cell type in your PSA doubling time is 15 months or more than active surveillance is fine. Here’s a good podcast on that.
If you’re responding to PD5 inhibitors continue to use those. If Trimix works for you keep going with that. But make sure that you stretch and oxygenate your penile organ or it will atrophy and shrink. You would be surprised at how much that will bug you. Good luck. Rick
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.