EDIT 2: Found New blood test where TSH is now up to 5.63 (only 3 months distance from previous test which showed 4.5!)
FT4 was 16 however which is within range.
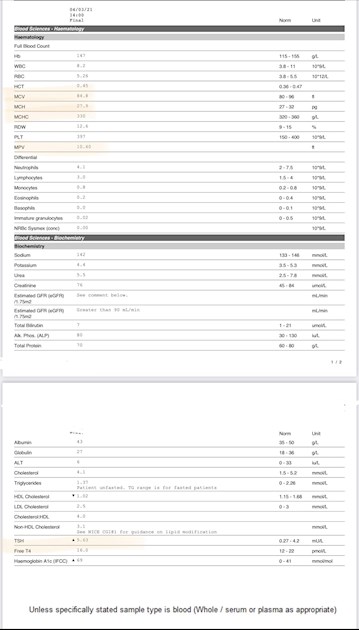
But also showed MCH, MCHC and MCV borderline which could be related to iron deficient anaemia apparently. Test pic below.
EDIT: oh wow!
This post definitely turned into something I did not expect (in a positive way).
So much information a fantastic resources and knowledge!
I have had so many symptoms of hypothyroidism/ Hashimoto and have never realised it. I’ve been dismissing some symptoms for a reason or another. I was also scared to bring some of my issues to the GP because in the past anytime I mentioned anything it’s loose weight, yet despite doing what needs to be done to be considered a realistic effort I can’t loose the weight! I’ve even tried medications they prescribe for the weight and they didn’t help (from metformin, to orlistat to GLP-1, etc).
I will definitely be advocating for myself and try to get the right blood tests and advocate for myself even if they think treatments is for levels of 10 or above.
Some of my symptoms:
- Fatigue (I sleep a minimum of 10hrs and honestly unless someone wakes me up even 12-14hrs - this is quite embarrassing!) and I still feel lethargic and tired, I can walk from the bed to the bathroom and my energy is finished.
- Anxiety/fight of flight responses for no reason ( I just start having that feeling something is about to happen for no reason)
- palpitations
- Depression : I have noticed it since last year (I don’t think the lockdowns had much a hand as I prefer to be alone and I’m not too social.. too many social interactions drain me)
- lots of mood swings, especially sadness, anger, etc
- Memory: I used to be very sharp and fast in my head. Now I struggle to remember things, I forget my words, randomly think something to do and not even a second later I forget, walk into a room and no clue what I’ve gone there for, etc.
- 50% Hair loss: I’ve lost about half of my hair, I can literally see through my scalp by looking at my forehead 😭😭😭, there were times I had to put my hair in a bun or loose braid (to avoid tangling) and only brush it once a week as every time I touch them huge chunks fall off 😱. This still happens.
- Numbness/ pins and needles in hands feet and lower arms and lower legs. (Doesn’t seem to be diabetes as sensitivity is very good).
- Headaches, lots of them
- no hunger
- no weight loss whatsoever and steadily gaining weight!!!!
- insulin resistance
And I’ve only just turned 28!
Feeling kind of scared and overwhelmed a little bit. Mostly because all of this could have been prevented most likely. Especially the psychological effects of all this and how they all correlate. For example when trying to be healthy and have good blood sugar control and despite all the effort nothing seems to work, or when trying to loose weight and again nothing is working, but doctors don’t put 2+2 together and see the underlying causes of things. I have traumas in regards to this that date back to the ages of 11 or so as I had PCOS since then (based on symptoms and my diabetes could not get controlled regardless of what I would do. And I would only get shouted at.
Sorry for the long rant!
It seems like trying for a baby in 6 months time is not happening afterall 😔.
———————————————
Hello!
I am very new, so I’m sure my question would probably be identical to many others! Sorry 😅
I have a few medical conditions which have been diagnosed such as Type 1 Diabetes and PCOS with severe insulin resistance.
But I’ve also noticed in my most recent blood tests (Nov 2020) that I’ve had a few things show up either being borderline or deficient, but the GP didn’t even mention them to me.
I’m asking them for new blood tests, but so far have been unsuccessful - hopefully will get new ones in the next 2 months 🤞.
I’m posting here as I’ve got my TSH level which was trending on the lower end for about 2yrs but it just crossed the upper end in the last results.
I have a lot of symptoms which are both related to Hypothyroidism, folate deficiency and PCOS.
I’ll also disclose I’m obese, as I know that affects these things too. I have a healthy diet and in the past 1 month switched to a Keto diet to control my diabetes, which works.
Despite being in a healthy calorie deficit and exercising, the weight does not shed.. but it’s likely to be connected with my poor sleeping habits and stress.
These are my results which I thought are worthy of note:
TSH 4.5mu/L
Serum Bilirubin 3umol/L (1-21)
Serum ALT 6-9iu/L (0-33)
B12 556
Folate 2.7 (3.9-26.8)
Ferritin 60ug/L (30-400)
Vit D 27 (30-200)
MCH 28.1 pg ( 27-32)
MCHC 328g/L (320 - 360)
Platelet 386 (150-400)
Sorry if some are not relevant 😬
What are things you would recommend looking into?
Any specific Blood test to request?
Any supplements to try?
Written by
OudMood
To view profiles and participate in discussions please or .
No, they are currently not treating either.They haven’t even addressed it in a convo at all.
I am now supplementing every other day (or daily when I can - I’m bad at taking pills hahah) with vit D3 4,000u. This should definitely resolve that issue.
I used to be prescribed 5mg folic acid previously but I recently tried to do a refill for Folic acid as I’m considering conception in the upcoming months (6+ months) so it’s time to become serious with folate but they refused as I “didn’t have it before” 🤦🏼♀️ - clearly in my notes and letters from consultant.
I’ll ask them to address it again.
What about the elevated TSH?
Ive been told that an optimal functional level is 1-2, but even based on the clinical it’s slightly elevated… 🤔
I am now supplementing every other day (or daily when I can - I’m bad at taking pills hahah) with vit D3 4,000u. This should definitely resolve that issue.
It may take some time to resolve Vit D deficiency with that level of dose.
At one time Vit D deficiency was diagnosed when the level was below 30, now some areas have lowered that to 25. But you can follow the NICE Clinical Knowledge Summary to treat this yourself:
"Treat for vitamin D deficiency if serum 25-hydroxyvitamin D (25[OH]D) levels are less than 25 nmol/L.
For the treatment of vitamin D deficiency, the recommended treatment is based on fixed loading doses of vitamin D (up to a total of about 300,000 international units [IU]) given either as weekly or daily split doses, followed by lifelong maintenance treatment of about 800 IU a day. Higher doses of up to 2000 IU a day, occasionally up to 4000 IU a day, may be used for certain groups of people, for example those with malabsorption disorders.
* Several treatment regimens are available, including 50,000 IU once a week for 6 weeks (300,000 IU in total), 20,000 IU twice a week for 7 weeks (280,000 IU in total), or 4000 IU daily for 10 weeks (280,000 IU in total)."
So you can decide yourself which way you want to do it, personally my maintenance dose is 5,000iu daily winter and summer, so 4,000iu would have done nothing for my Vit D deficiency.
Decide how you want to start dosing but make sure that you get the loading doses of 300,000iu fairly quickly. Once the loading doses have been completed you will need a reduced amount so you should make sure that you are retested after you have finished the loading doses so that you know how much you should then take going forward. Post new result on the forum for suggestion of appropriate new dose at the time.
The Vit D Society and Grassroots Health recommend a level of 100-150nmol/L, with a recent blog post on Grassroots Health mentioning a study which recommends over 125nmol/L. Once you've reached this level then a maintenance dose will be needed to keep it there, which may be 2000iu daily, maybe more or less, maybe less in summer than winter, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. This can be done with a private fingerprick blood spot test with an NHS lab which offers this test to the general public:
Doctors don't know, because they're not taught much about nutrients, but there are important cofactors needed when taking D3. You will have to buy these yourself.
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking D3 as tablets/capsules/softgels, no necessity if using an oral spray.
For D3 I like Doctor's Best D3 softgels, they are an oil based very small softgel which contains just two ingredients - D3 and extra virgin olive oil, a good quality, nice clean supplement which is budget friendly. Some people like BetterYou oral spray but this contains a lot of excipients and works out more expensive.
For Vit K2-MK7 I like Vitabay or Vegavero brands which contain the correct form of K2-MK7 - the "All Trans" form rather than the "Cis" form. The All Trans form is the bioactive form, a bit like methylfolate is the bioactive form of folic acid.
Magnesium helps D3 to work. We need magnesium so that the body utilises D3, it's required to convert Vit D into it's active form, and large doses of D3 can induce depletion of magnesium. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking magnesium as tablets/capsules, no necessity if using topical forms of magnesium.
Unfortunately, as we are never tested for a baseline in health, none of us know what our own "normal" is.
Is your TSH currently above range? A TSH of over 3 is the trigger for a diagnosis of hypothyroidism and treatment in some countries, in the UK we need TSH to go over 10 for a diagnosis of Primary Hypothyroidism.
You also need FT4 testing, just testing TSH on it's own is inadequate because it misses cases of Central Hypothyroidism where the problem lies with the pituitary or the hypothalamus rather than the thyroid, and the TSH doesn't rise because the signal isn't being sent from the pituitary, but the FT4 is low.
You are unlikely to get full testing from your GP, especially at the moment due to the shortage of blood tubes and GP practices have been asked to suspend non-urgent blood tests for the time being. You can do a private test with one of our recommended labs and this can be done by fingerprick which uses very small tubes requiring less than 1ml of blood.
I would choose a test that includes TSH, FT4, FT3 and thyroid antibodies, eg Medichecks Thyroid Function with Antibodies test or Blue Horizon's Thyroid Premium Silver.
Hi, I had a follow up question..Can I just easily ask the GP to prescribe the loading dose of vitamin D or am I supposed to do it with over the counter pills?
As that could mean something like 11 tablets x 4,000ui a day for over a week just for the loading dose 😳
As that could mean something like 11 tablets x 4,000ui a day for over a week just for the loading dose
No it doesn't. If you look at the NICE Clinical Knowledge Summary that I've quoted above, the loading doses total 300,000iu over a number of weeks and they give examples of how GPs can do this. Nowhere does it say 44,000iu a day for over a week. It says
"Several treatment regimens are available, including 50,000 IU once a week for 6 weeks (300,000 IU in total), 20,000 IU twice a week for 7 weeks (280,000 IU in total), or 4000 IU daily for 10 weeks (280,000 IU in total)."
Can I just easily ask the GP to prescribe the loading dose of vitamin D or am I supposed to do it with over the counter pills?
Has your GP not already discussed this result with you? Considering that your result is below the given range then it's pretty negligent of your GP if he hasn't brought this up.
Depending on what your area classes Vit D deficiency as, if it's <25 you wont get loading doses, if it's <30 you should get loading doses, your GP may or may not prescribe them. Your GP should prescribe something even if your 27nmol/L is not classed as Vit D deficiency in your area, in which case you can top up what they give you or just go it alone. The choice is yours. You could quite safely take 5,000iu yourself as long as you retest in 3 months then adjust dose according to your new level once your reach 100-150nmol/L.
I would say, though, that you will get a better D3 supplement if you buy Doctor's Best (my choice of D3). I take 5,000iu D3 daily as a maintenance dose and I've just paid £16.99 for 360 so that will last me a year (720 cost £26.99 so even better value).
* Blood draw no later than 9am. This is because TSH is highest early morning and lowers throughout the day. If looking for a diagnosis of hypothyroidism, an increase in dose of Levo or to avoid a reduction then we need the highest possible TSH
* Nothing to eat or drink except water before the blood draw. This is because eating can lower TSH and coffee can affect TSH.
* If taking thyroid hormone replacement, last dose of Levo should be 24 hours before blood draw, if taking NDT or T3 then last dose should be 8-12 hours before blood draw. Adjust timing the day before if necessary. This avoids measuring hormone levels at their peak after ingestion of hormone replacement. Take your thyroid meds after the blood draw. Taking your dose too close to the blood draw will give false high results, leaving any longer gap will give false low results.
* If you take Biotin or a B Complex containing Biotin (B7), leave this off for 7 days before any blood test. This is because if Biotin is used in the testing procedure it can give false results (most labs use biotin).
These are patient to patient tips which we don't discuss with phlebotomists or doctors.
If you want to do a fingerprick test and would like tips on how to do this, please ask and I will list them for you.
I wouldn't bother having doctor's comments from the private labs, they tend to just follow what the GPs say and put more importance on TSH than the actual thyroid hormone levels. If you put your results on the forum, with their reference ranges, you will get a better intepretation here.
Wow!Thank you so so so much for taking that much time to type all of that out! ❤️
I definitely need to look into this way more, even just the vit D alone!
I thought 4,000 u were sufficient as I was always deficient and a Gp yrs ago told me that taking 1,000u would be sufficient, then said that I may need 2,000 (as values weren’t improving much) but then nothing.. but clearly I was very ignorant!
Thank you so much again for all of this and the resources! I’m screenshotting all of this! 😬
Good chart there too about levels required to prevent many illnesses. Please note the different measurements - ng/L is used in the US and elsewhere - in the UK it is nmol/L. They often post both !
Testing TSH isn’t sufficient. Once it’s over range the lab should automatically test thyroid hormones, but this wasn’t done?
FT4 & FT3 are the actual thyroid hormones but GPs look at the TSH. A Normal TSH is around 1. Yours is high. The TSH is a pituitary hormone. When it starts rising it attempting to get the thyroid to produce more hormones and it happens when levels are low.
Another thing you should have tested is thyroid antibodies. Thyroid Peroxidase (TPO) and Thyroglobulin (Tg) this will show if your thyroid is being attacked by your own immune system.
You could ask GP but if they refuse you might have to use private blood testing companies.
Folate and vitamin D are below range your GPs should be treating deficiencies but you may find they only bring levels into range and then do not recheck. What medicines and supplements do you currently take?
Thank you for such an in depth explanation.No I’ve looked a few times to see if those were present and already noted down to request T3, T4 and FT4I..
My TSH had an upward trend for the past few years but no one ever mentioned it.
To be honest even now with it being above the limit and being flagged as abnormal I wasn’t told nada. 🤕
TPO and Tg were definitely not tested, well nothing concerning Thyroid was other than TSH.
I hope they would take it more seriously due to the higher risk factor of PCOS and T1D. I did hear about the correlations with stuff like Celiac disorder, Thyroid, etc. They diabetes team used to be involved in that before but not anymore it seems as no one mentioned it to me for at least 7-9yrs on the diabetes team side of things.
I was also in a normal weight with BMI under 18.5 until 17, and then increased to about 23-24 and after 20, when I was finally diagnosed with PCOS I was put on Dianette a combined pill and was not followed up (as the guidance says to review in 3 mo) and have started gaining weight, a lot of it all of a sudden and it just skyrocketed from there with my BMI now being 43 and not loosing weight despite always being in calorie deficit (unintentionally, as I’m often not hungry..).
Im mentioning as I remember reading somewhere it is related somehow sometimes.
I’ve switched to a Keto diet recently and it helped a lot with my Blood sugars and my estimated a1C is now 32 from approximately 65.
(Good range to strive for is 42-48, and anything under 42 I believe is non diabetic!)
But weight isn’t moving at all. I’ve initially lost 4kg and then nothing (in fact I’ve regained about 1.5kg of the initial loss). And I’ve done all of the troubleshooting etc so it’s not overeating, or not being in ketosis, as my blood ketones are regularly 1.5-2.5.
Ive recently started the following (about 2-3 weeks ago):
Your GP can request thyroid hormones but often labs are set up to automatically test TSH and FT4 only if TSH out of range. Testing FT3 & antibodies are often refused.
There is a total thyroxine (T4) and total triiodothyronine (T3) but these aren’t useful measurements you need to know the unbound usable levels FT4 (the free thyroxine) & FT3 (the free triiodothyronine)
There also Reverse an inactive form rT3 but this isn’t a useful measurement. Make sure the right things are requested.
It can be pretty shocking the things GP overlook and do not offer advise on. Getting your own results and checking what’s being tested and the results is a habit you must keep to.
Type 1 diabetes and autoimmune thyroiditis are both autoimmune. There are associations with PCOS and celiac. It sounds like your doctors are not monitoring you very carefully.
Poor appetite can be a hypothyroid symptom.
How may carbs & calories do you have per day? I am overweight and did 1000cal and 80gcarb for 6 months last year for weight loss, when I was diagnosed type 2 with a Hba1c of 51. GP said “reduce carbs” that’s all the help I was offered! Within 6 month was 35 & 1 year was 30.
I have hyper so reducing levels was helpful to me, but after 6 months it was beginning to show in the FT4:FT3 conversation. Too few calories and carbs may be affecting how well the FT4 converts to FT3. The FT3 being the most active hormone.
Keto may be too restrictive. You need the right level calories & nutrients or this will make matters worse not better.
HbA1c measures the sugar attached to the haemoglobin, so it gives an average reading from past few months.
I go by this range
* HbA1c below 41 mmol/mol (6.0%): Non-diabetic
* HbA1c between 42 and 47 mmol/mol (6.0–6.4%): Impaired glucose regulation (IGR) or Prediabetes
* HbA1c of 48 mmol/mol (6.5%) or over: Type 2 diabetes
It likely varies for type 1 and usually a aim is set for you?
Supplements containing high levels of Biotin (B7) can skew test results. Check labels & avoid 1 week before draw. When you test do you test early in morning after fasting except water? This give highest TSH & lowest FT4. Doctor often think this is not relevant and don’t advise about this.
Calories wise it kind of depends. Now I’m forcing myself to eat in the range of 1,200-1,400 calories otherwise I’d sit happily at 1,000. I just don’t feel as hungry.
Keto is fine for me, I don’t feel restricted as such, especially because I find that my blood sugars are impossible to manage if I eat more carbs than this (I sit comfortably at 15-30g a day). Things just skyrocket from Bt here and insulin demand goes through the roof. The moment I went on keto within 4 days my insulin demand more than halved! (And it wasn’t food bolus insulin, but background insulin mainly.)
I used to have an a1C going up and down between 80 and 68. With average BS of 9.5 when. I was really trying hard.
Now I’m sitting comfortably 5.1-5.5 average with predicted a1C of about 32.
My a1C aim was set initially at 48, but since my difficulties my doctors were happy if I even reached 54-56 as they could see the struggle.
But really if you’re in the 42-48 range it is deemed to be excellent blood sugar control.
But removing carbs allows you to remove blood sugar spikes, which makes it easier to have better control.
I will definitely push for all the tests above and keep insisting of the list of symptoms and the strong correlation between T1D, PCOS and hypothyroidism. I now have a better GP than before and she’s more up to date with things and I’ll see what she say. Often is having the wrong GP at your appt that is an issue, so I’ll ask to speak to the nice one 😂.
Thanks for the tips.
I don’t test very early in the morning, but I usually fast as I don’t really eat breakfast anyways.. 😬
Full thyroid testing is needed to include the FT4 - FT3 and Thyroid Anti-bodies TPO & Tg which I doubt your GP will carry out. Private Testing is available through Thyroid UK - testing kits sent to your home. Special Offers on Thursdays !
Thank you.I will be asking to get those tests done.
I had already written T3, T4 and FT4I as recommended in the NHS website, but will also add TPO and Tg due to my autoimmune situations 😅.
I hope they can do it as finances are in the tighter side with all of these supplements and other diabetes extras I need wich are not NHS funded 🤕. (£200 per month on the diabetes alone… 🤦🏼♀️).
I’ll look into the hashimoto relationship as I’ve heard of it and remind the GP of it if they refuse..
Unfortunately even if your GP was helpful enough to request those tests - it is the lab that will not test if the TSH is in range. Also the NHS rarely test the Anti-Tg. It is very frustrating but reading around the posts/replies here you will see it is common place. Request your GP adds a special note on the Blood test request.
1000's of us here have to test privately in order to find wellness with the correct testing. I have been reading here since 2011 so have a reasonable grasp of the difficulties ! I really hope your GP listens to you ....
Yes it is costly - I agree. I buy my own Thyroid meds and B12 injections on-line plus all the supps for hubby and myself - we both have Hashimotos. We are pensioners but value our health .... don't forget the Special Offers flagged here on Thursdays in the News Feed 🌻
Thank you so much. I hope my pre existing conditions may give me a better fighting chance. As I also have the option to discuss this further with my new endocrinologist (recently switched) which is very advanced so may be more interested in testing all of that… I hope at least.
I think this gives me a slight advantage (or at least it did in the past when I needed extra tests/care).
Going to the Endo appointment without up to date blood tests seems to me to be a waste of time. I would 'invest' in them before you go so you have something to discuss on the day. If he tests at your appointment then it's more time wasted waiting for results to you and the GP - and yet another GP appointment. What a crazy system ? !
That’s what happened when I went. They took lots of blood tests at 3pm and I had taken my thyroid meds that day too. Then had to wait 10 weeks due to christmas closing for the results and then another 4 months to go back and see him. This was all before I knew a thing about thyroid issues and had found this forum.
I think it should be mandatory for everyone to go on healthunlocked before they see any specialist, just to make sure they ask the right questions and have the right info available to make their case.
As you have double diabetes your GP should really be doing everything to help you. Keep in touch with them and read up on Diabetes UK about this rare condition. Keto can be hard to stick to, I found LCHF much easier and very effective. With either of these types of weight loss you do not look at calories. Lots of weight loss support on Diabetes UK from those who fully understand.
Make sure you keep on top of nutrients, your GP really no address the deficient folate.
Yes it’s the insulin resistance with T1 . I found this on Diabetes UK, I had a quick look earlier I had heard of this before so before commenting I looked it up:-
Double diabetes is when someone with type 1 diabetes develops insulin resistance, the key feature of type 2 diabetes.Someone with double diabetes will always have type 1 diabetes present but the effects of insulin resistance can be reduced somewhat……….
Someone with double diabetes will need to keep taking their insulin every day as their type 1 diabetes will always be present.
In addition, they will need to try to combat the insulin resistance by adapting their lifestyle to help regain their sensitivity to insulin and slowly and safely reducing the amount of insulin they take.
Eating foods with fewer carbohydrates and a higher fibre content can be effective. Including more exercise into one’s daily routine can also help to increase insulin sensitivity.
Medication usually prescribed for type 2 diabetes may also be prescribed to help improve insulin sensitivity as well as to aid weight loss.
There is a lot more info on the site, however if your GP and/ diabetic nurse do not understand tell them where this info is so you are properly treated.
What a nightmare for you. I hope you get the help you deserve/ need.
Oh I see, so rather than seeing the endo to get the blood test, I should get blood test from GP or private and go to Endo with findings.. correct?
A1C is good now that I’ve changed diet and significantly reduced carbs. Predicted a1C is 32 (5.1%) and it’s only recommended to aim for 48 (6.5%) so that’s good
I wonder if treating the hypothyroidism may help weight loss 😬?
Hi, glad to hear you are going to advocate for yourself now. But please get private tests ordered today to see your T3 t4 and tsh plus antibodies - then you’ll know your baseline and can start levothyroxine. Nhs never tests T3. Also do start taking methyl folate once you’ve tested your bloods. You won’t feel well till you do. My folate always dips low when I am hypothyroidi.
I had sub clinical hypothyroidism at your kind of levels but nonetheless a lot of symptoms which hit worse over the years despite taking Levo. I had to really build up meds to get my T3 high in range til I felt better and stopped gaining weight.
Do you know how to do that? As my Gp gives printed digital forms, but when I go to to the phlebotomist they throw that paper eventually and just have the sticker on the vials…So even if they write it on the paper… the lab won’t see it..?
Lol sorry, I’m sure the GP would do it just want to make sure I insist on the correct thing 😅
Mine are all electronic so she must put it on the electronic request which of course I cant see. She told me the lab told her to write that so they'd do all 3 tests: TSH Ft4 & Ft3.
Morning, I haven’t been on here for a long time but you’re post caught my eye because you’re describing a lot of Cushings symptoms which doctors usually misdiagnose as pcos- The weight gain to no avail losing it has anyone mentioned this to you regarding Cushings? If not you need to ask to have you’re cortisol levels checked which don’t always come up with a high reading if that’s the case you ask for 4 -1each week to be tested also midnight salivas and bloods . There’s syndrome ( adrenal) and disease ( Pituitary) This is a very complex disease which affects everything including bone deterioration if not detected earlier rather than later-Panic attacks anger due to high cortisol and insomnia which you didn’t mention there’s so much more I could tell you as I’ve had Cushings and you have to advocate for yourself very sternly unless you have a very good doctor and Endo I wish you luck on getting a solution.
Wow! In my 40s I had terrible gushing periods, thick pubic hair and facial hair, difficulty concentrating, depression, and weight gain. Back then, PCOS had not yet been invented, so I was diagnosed with low estrogen and started on HRT. That cleared up the bleeding problem, but not much else. I have also been told that I have a "male pattern output" of cortisol (24 hour collection of urine). So I suppose that means it was high for a female but still within range if I had been male instead of female. No treatment was offered.
Hi I’ve never heard of that a male pattern re cortisol I swear some endos make this stuff up! If you are still having symptoms I think you should go back to you’re GP abd ask for testing as something drives the cortisol you shouldn’t have been left if it was high.
Hello. You already have a lot to research and think about but here’s another one! A few days ago another member posted this link which I thought was fascinating as my daughter has put on a lot of weight and just can’t shift it. It’s all to do with women, weight gain and iron and you certainly seem to be deficient in iron. Definitely worth a watch. healthunlocked.com/thyroidu...
Thank you so much for the link! It certainly seems an interesting video!
I haven't read through all the answers to you. Have you ever had your cortisol levels checked? Is your weight mainly around your abdomen? Some of your symptoms point to Cushing's Syndrome, especially not being able to lose weight. Was your PCOS diagnosed by blood tests or scans? Often PCOS is misdiagnosed & it may be Cushing's syndrome although you can have both. This chart shows the symptoms of Cushing's, see if you have many of them.
Thank you!You’re the second person mentioning this to me.
I definitely do have PCOS as I’ve had numerous scans including internals and they have always had PCOS characteristics, since puberty and was relatively fit till about 20 or so..
Just to understand with my values are you suggesting that I have Cushing instead of PCOS or Cushing instead of Hypothyroidism?
Would Cushings elevate TSH?
I haven’t had my cortisol tested ever, but I have definitely been very stressed almost constantly for the past few years.. as I have a long legal battle which is draining a lot of finances and we’re litigating finances in the 6 figures… so that hasn’t helped for certain.
Hi Cushings elevates everything unfortunately cortisol is in nearly every cell and as Pauline said PCOS is often misdiagnosed in actual fact a lot! So many women have to fight for a diagnosis so the earlier you now get on top of this the better people go undiagnosed for years it affects cholesterol liver enzymes to name but a few but because a lot of doctors don’t understand Cushings they don’t get it you need a Cushings expert if you need any help give me a shout I’ll do what I can as will Pauline.
Well.. I’ve attached a picture that came up while looking at Cushings. It’s basically me, just change the hair. (I’m not even joking or exaggerating that’s how I look! - maybe thicker legs and arms a bit and not so much with the bruising)
I’m feeling very anxious and stressed since yesterday. I feel like I hit a brick wall and all these new things are happening.
I may manage to get an emergency appt with my Gp tomorrow, so I wanted to ask a couple of questions.
1. Could Cushings co-exist with Hypothyroidism/Hashimoto?
2. Could Cushing elevate TSH (mine in March was 5.63mu/L)?
3. What tests should I request to diagnose or exclude Cushings?
If you are Facebook I run a support group for those whoo are looking at Cushing's, it's called Cushing's UK. It;s made up of people who are testing, those waiting for treatment & those is remission from it. So you will get a lot of help & support as to the tests & how to approach your GP. facebook.com/groups/2207009...
Yes Cushings can coincide with hyper parathyroidism also but you don’t want brain overload at this point the main thing is urines bloods midnight salivas as said urines don’t always test positive the first time hence the other testing and repeated urines if necessary- There are groups you can request to join as Pauline said the Uk one but also Cushings support-,and the many faces of Cushings their are literally thousands of people to help you along with this x
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")