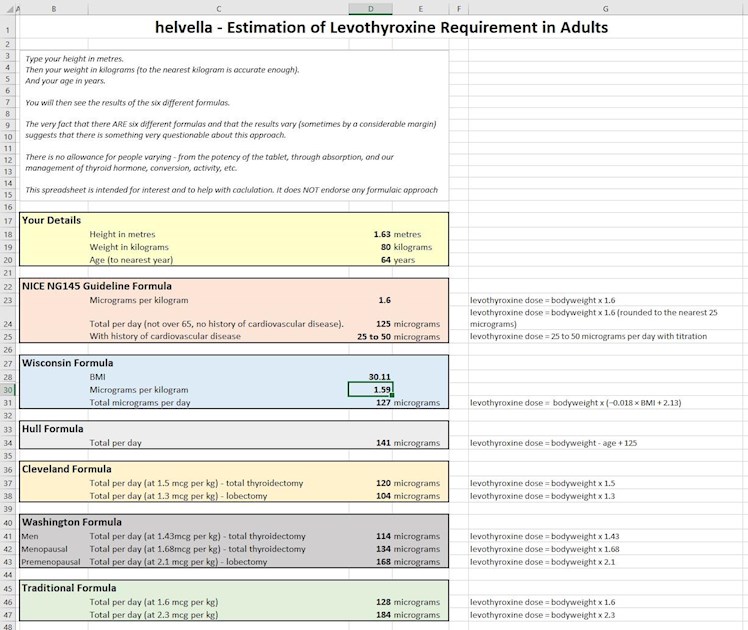
Years ago, I created a spreadsheet for calculating levothyroxine doses using various formulas.
I have, at last, got round to making a few changes. The most significant is that I have added the formulas used in the NICE NG145 Thyroid disease guidelines. It has also been renamed.
This replaces the old spreadsheet which will no longer be available.
I still consider that putting a number or three into a formula is a very poor basis for dosing. Other factors need to be considered. Further, the NICE formula would mean there can be dramatic changes in dose just because you hit your 65th birthday before diagnosis. (They change from a weight-based calculation - maybe 100 or more micrograms to "25 to 50" micrograms.)
helvella - Dosing by Age and Weight
A document which discusses the issues of dosing by formula at greater length.
Certainly, if the NICE formula works out to imply that you need a higher dose than you are getting, it could be a tool to get that dose increase.
But there is a cost to such formulaic approaches.
Other people will be mis-dosed by some doctors blindly following the guidelines.
How many will not get an increase because they are already on the dose the formula implies? Never mind that they have, for one example, gastroparesis and therefore very poor absorption.
How many will be put in an excessive dose because the formula implies a higher dose than they need? (There is an implicit assumption that the patient has zero thyroid function in the NICE approach.)
How many will have their dose reduced because they manage to lose weight? Many GP surgeries encourage weight checking at appointments. It could be a nasty surprise to find your dose suddenly cut by 25 micrograms.
How many actually need some T3 rather than an increase in levothyroxine? (In such people, extra levothyroxine could be to their detriment.)
If you accept formulaic dosing, you also rather accept that FT4 and FT3 tests are unnecessary. There will be a tendency to at most run a TSH test just to check that isn't too far out.
If TSH is way out, high or low, this formulaic approach leaves everyone cast adrift without a compass.
We have to push for consideration of symptoms, with FT4 and FT3 to help, as the primary approach.
I consider that a formula can be useful to indicate a starting point. Thereafter, only as a "sanity check" on dosing.
Couldn’t agree more, I am glad you pointed out the absurdity of it - how can you possibly one day need 100mcg and the next just 25mcg - all because it’s your 60th birthday - how utterly nonsensical is that & I don’t think much of NICE’s idea of a birthday present. Did they turn off their brains when they were concocting this stuff or do they actually have any brains at all? I’d call it an insanity check in this case.
Ahhhh so how is this going to help patients with hypothyroidism??? Its just plain bonkers. What is the matter with the thyroid world of endocrinologists and doctors? Are they all so severely hypothyroid they are suffering with dillusions? Honestly they all need sectioning!!
So lets see- the latest advice is you cant have treatment unless your TSH is over 10 then you can have treatment without any follow up tests by body weight and age? And then miracoulosuly when you hit 65yrs you need a quarter to half less of thyroid meds of what you had before? You just couldnt make it up could you? At the back of this is a money saving exercise and absolutely nothing to do with optimising and treating the poor s*** ( excuse my language) who have the misfortune to have hypothyroidism. We can all look forward to further suffering with the knowledge that weight gain will increase thyroid meds but weight loss will decrease thyroid meds forcing many of us to become and stay obese. Marvelous! Cant wait! Oh and Im on the brink of turning over 65 - further joy to behold and if this is implemented ill health and a shortened life. Thanks NHS. Should nicely solve the problem of us all living longer!!
Like many of the protocols for hypothyroid treatment on the nhs.....no logic at all. Sorry Helvella my anger is definitely not aimed at you at all as I always appreciate your posts but the beurocratic nonsense that stops patients being treated.....let alone optimally treated. Its just gets more insane by the year. And of course will force more and more people to go off piste or stay & become ill. Am struggling to think what the plus side is of this......
Interestingly, if I average all the applicable numbers to me I get quite close to the dose I’m on (which I think is around optimal but TBC with adrenals). Not sure what that means realistically aside from that no single one is useful in isolation. Which of course we already knew about numbers without considering the full clinical picture!
I have just added a quote to the discussion document linked earlier:
Levothyroxine Therapy in Thyrodectomized Patients
Conclusion
Despite a remarkable commitment by researchers to find a therapeutic scheme able to predict the exact dose of LT4 to be given to patients after a total thyroidectomy, the attempt to reach the precise dosage failed to reach the target in the totality of the cases. It is reasonable to conclude that because most of the schemes show a considerable complexity but do not offer significant advantages in the percentage of patients reaching the expected results, the search for a fully predictive model seems to be an exercise of futility. Nonetheless, these schemes are of great utility to start the replacement therapy approaching the best dosage, but keeping in mind that changes during follow-up can be necessary according to the TSH values that are to be reached in every case.
Miccoli P, Materazzi G, Rossi L. Levothyroxine Therapy in Thyrodectomized Patients. Front Endocrinol (Lausanne). 2021;11:626268. Published 2021 Jan 29. doi:10.3389/fendo.2020.626268
The weight calculation one put me in the right area too but I needed more T3 which the Levothyroxine alone could not deliver and no amount of number juggling would make me feel better (I have DIO2 genes for poor conversion of T4 to T3). If only they would accept that how you feel is actually the BEST indicator of optimisation not a load of arbitrary formulae and numbers, things might massively improve for patients forced to endure this preposterous situation at the considerable cost to their health and the economy.
Thing is I really dont think they are remotely interested in optimal dosing.....just the lowest amount they can get away with.....anything to save money. The fact is, when treated like this, is that you end up on a ton of other medications because of the suboptimal treatment which costs far more!!! For supposedly intelligent people in the medical world there is very liitle thinkng that goes on!!
Thanks for this useful compilation Helvella. My mum who turned 80 last month has just been started on 25mcg levothyroxine- her TSH was 6.5 in January and 8.6 in March and given 2 of her daughters are hypo (me included) & one is hyper (graves diagnosed 2 years ago) I had a feeling she needed some thyroid hormone.
The issue is she had a massive heart attack 8 years ago so I’m wondering how safe Levothyroxine will be for her especially if dose needs to increase? After 2 weeks she feels a bit better- less sleepy in the early evening & less muscle ache.
Perhaps it makes sense to look at it from another point of view? This isn't supposed to be an evaluation of your mother's health and needs - just an observation.
Having insufficient thyroid hormone in your body causes damage to all your organs. Many people who become significantly hypothyroid lose muscle mass. The heart is largely muscle.
When it comes to dose, she will need what she will need. If she needs more, whether 50, 75, 100 or any other amount, then getting that dose can be expected to make her better than being left on an inappropriate dose. Steady, thoughtful adjustments, with sensible gaps and sufficient testing (not just TSH) - very much taking into account how she feels - is likely the best approach.
Thanks HelvellaThe only reason for asking about my mother is because the NICE guidelines suggest if there is a history of cardiovascular disease the disease of Levo should be 25-50mcg & not increased.
You make a good point about loss of muscle mass with hypothyroid & heart being a muscle. I’d never thought of it that way. Explains a lot.
Consider starting levothyroxine at a dosage of 25 to 50 micrograms per day with titration for adults aged 65 and over and adults with a history of cardiovascular disease.
So increases are perfectly reasonable within that! Titration could take it up to any level.
I had been perfectly well on the same brand for years then given another brand I now have a autoimmune disease through this so don’t know if it was a stronger one or weaker one so have these guidelines took this into account with all the different brands.
Of course the guidelines don't take account of different makes!
For a start, the pharmaceutical view is that the various makes are sufficiently similar that they are equivalent.
Am not sure what you mean about autoimmune disease - it is very likely that having autoimmune disease is why you had a thyroid problem.
Most incoherently, you can read that levothyroxine oral solutions are better absorbed than tablets. Yet these formulaic approaches don't even try to take that into account.
Interesting, and in the ballpark of what my GP keeps saying that I should take, making me think that she is using a formula like this (but not just for identifying an initial dose). However, for me, I feel completely hyper and horribly unwell if I take anywhere near the dose that those formulae suggest. In practice, I take between a third and a half of those values, with my resulting bloods (FT3, FT4, TSH) at or very close to where they want to be (caveat - this was the case pre-pandemic, I haven't had a full set of thyroid-related bloods done this last year). Such simplistic formulae might be ok to suggest an initial dose, but I'd be very wary of using them for anything more than that.
I can understand how someone could look at blood tests and suggest a change of dose - more or less depending on the actual values.
When driving on a clear road, we would usually keep a steady speed - the speedometer informing us what speed we are doing now. If our speed drops, we very slightly increase the pressure on the accelerator pedal. If our speed rises, we very slightly reduce the pressure.
We don't say that the accelerator pedal should be depressed one third the way. And it would be a nonsense as in one car that might mean 50mph and in another 120mph!
That is, adjust the dose, moderately and thoughtfully, to move in the direction required. Don't come up with some number, a "magic" number, as a target dose to take.
Brilliant! However this would require some application of use of brain for doctors - for most doctors where hypothyroidism is concerned their brains withered and faded away years ago.....they are not allowed to think but simply look at their screens and follow that irrespective of what/who sits infront of them! Ive been thinking of sending my dog in with a pre-recorded message......am sure the outcome would be the same........providing they didnt weigh my dog!!! 🤣😀😉
Especially as even the NG145 guidelines expressly point out:
Be aware that the TSH level can take up to 6 months to return to the reference range for people who had a very high TSH level before starting treatment with levothyroxine or a prolonged period of untreated hypothyroidism. Take this into account when adjusting the dose of levothyroxine.
However, the obvious inference is that TSH will not only be within the reference interval but also that it will reflect the thyroid hormone levels in pretty much exactly the same way as it does in those with no thyroid issues at all. Which is unproven in general let alone in the individual.
Similar arguments apply post RAI and post-surgery.
Dear Helvella, very interesting your spreadsheet. As I am 73, it said that I should be on a very low dose. As you say, this is not a formula, but in fact I think that on 100mg levo and 10 mg lio and I may still be undermedicated. It is such a puzzle. Thank you so much for all your information that you put out. Susieibbo301
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")