I started on ndt in July and have my first lab results.
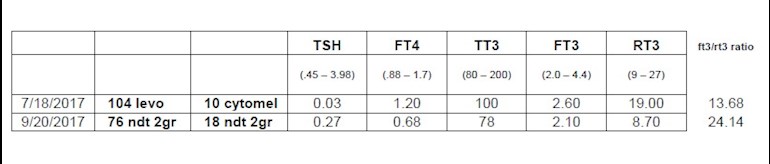
Please see photo for ranges/details.
fT3 dropped from 2.6 to 2.1 and fT4 dropped from 1.2 to .68
So, you would be thinking how dreadful I must feel now? But I feel great for the first time in a long time!
The ft3/rt3 ratio went from 13 to 24. So, I'm sold on the ratio being a big part of the equation. I know that there is disagreement about this, but this is my experience.
Oh, and endo is upping my dose to 2.5 grains...
Written by
Kell-E
To view profiles and participate in discussions please or .
Actually, you did give an opinion regarding rt3 in my first post on this forum.
You said that I don't have an rt3 issue because my rt3 was mid-range.
Please do not respond to my posts if you are unwilling to do the research.
Scottbnk,
rT3 is mid-range so you don't have a rT3 issue.
TSH was suppressed, FT4 is less than halfway through range and FT3 is only 25% through range but FT4 and FT3 will change now you are taking NDT. FT4 will almost certainly drop, perhaps even below range but as long as FT3 is good around 3.4 - 4.4 it is fine. FT3 in the upper range usually means TSH will be suppressed.
B12 437 is unlikely to be deficient but if you have symptoms of deficiency in b12deficiency.info/signs-an... go to healthunlocked.com/pasoc for advice.
VitD 37ng/ml is sub optimal. Optimal is between 40-60ng/ml so you may want to supplement 1,000iu D3 daily.
What is it you don't understand about "I have no opinion about rT3/FT3 ratio"?
Interpreting a rT3 result within the lab ref range as normal is not the same as interpreting rT3/FT3 ratio.
I remind you that "This is a patient to patient forum and no one, including the Admin team, on this community should be assumed to have medical training of any sort.
Everyone is only speaking from their own experience, that of friends/family or other people they may have spoken to."
Please remind yourself of posting guideline #6 when you respond to members.
Great! Thanks, Scott. Just what I needed as a clarification.
The short answer to your question is a big YES!
I looked at your RT3 levels in July. 19 is a very high level and indeed you'd feel awful with those levels.
Rule of thumb: when we look for the optimal T3, the levels ought to be at the higher end of the range.
The same is reversely applicable for RT3. They ought to be nearer to the lower end of the range.
In general, as you probably know, in the event of too much T4 circulating in the blood, RT3 acts a break to protect the body from a surge of T3.
Previously, 104 mcg of Levo + 10 mcg of readily made T3, as your daily dose, was way more than what you needed and have prompted high RT3.
By lowering your dose to 2 grains of NDT (lower T4 and lower T3 from before), you have lowered the substrate of T4, and accordingly, your total circulating levels of T4 dropped as well.
Now, with the new levels of RT3 being under 9, your body is relieved and has ceased to be in the fight mode (RT3 increases Cortisol) as when it was on the higher dose and was able to flush the excess of RT3.
By doing so, your T3 levels however they may have been reduced, they are now actually reaching your cells whereas before all high levels of RT3 were sitting on the receptors and preventing the T3 from entering the cell.
You are on the right track and the little increase to 2.5 grains will hopefully make you feel even better.
Finally, if I may add, to maintain low levels of RT3, you have to have good circulating iron in your blood. Low iron or anemia will cause your body to make more reverse T3 than T3.
Low levels of Vitamin D, B6, B12 selenium, Zinc, and inflammation can all cause High Reverse T3 as well.
We are definitely on the same page on this. Just a couple of comments.
I have made sure that my D, B6, B12, selenium, zinc, and iron are being adequately supplemented. I have had problems converting for a long time and made every effort to eliminate these causes.
As for the change to 2 grain NDT...My ingested T4 went from 104mcg to 76mcg, which is a reduction. My ingested T3 went from 10 mcg to 18mcg, which is an increase.
My lower serum levels of T3 may be attributable to an overall reduction in converted T3 + ingested T3. Or possibly, as you mentioned, now that T3 is actually able to occupy receptors previously occupied by my former abundance of rT3, serum levels drop because those molecules are taken out of circulation. Yippee!
Everything you said is spot on. Now, is there any cold hard research that we can back it up with?
Did you take the labs for each med at roughly the same time of day? For example, did you take 10 mcg T3 one morning with your levo, and then test the next morning, 24 hours later? And same with the NDT? If not, what was the difference in lapsed time from taking your dose to testing?
Yes, plenty is out there. This resume is a synthesis of lots of reading and analysis.
I will do that extra mile for you and we'll try to compile a few easy readings and direct message them; only to for you to rest assured.
How about that for a deal/help?
Keep up those levels checked and topped up when needed. Have you been taking any selenium? something for you to consider adding to your daily cocktail if you have not been doing so.
As for your additional comments.... it is the too much of T4 that is the problem and causes RT3. Other than the conversion issues, it is a major reason as to why many patients do not do well on T4 alone. Overall, NDT is also known to reduce RT3.
You are on the right track with your endo! Keep him/her
I do not subscribe to the theory that rt3 blocks receptors for lengthy periods of time. It doesn't need to, as you body keeps making more each time you too much t4 in your mouth.
But it does make sense that rt3 competes with ft3 for receptors.
Then it is a simple matter of math as to what your chances of getting energy to your cells is. (depending on the affinity for receptors, which is being debated?)
But there are people out there that believe that rt3 does not occupy t3 receptors...that rt3 has receptors all its own. (in the liver, but that's a whole different subject)
There are people that believe that rt3 is simply a disposal pathway for t4 and that it has no other negative impact on cellular activity than the absence of the t3 it didn't become during conversion.
Greygoose, 20 days ago, presented some accurate and similar information:
“This is done by removing the 'wrong' iodine atom, so that the rT3 molecule is a mirror image of T3 - hence the name: reverse T3.
The rT3 molecule cannot get into the cells, meaning that the body has less T3 and therefore has to slow down. This is a normal safety procedure to preserve life.”
Separate from that here is my reply and I shall use exactly the same tool/link presented by the previous poster.
By definition, a "mirror image" or object which is identical in form to another, but with the structure reversed, as in a mirror. (Note the word reversed).
Now, let's examine the molecular structure of T3 and RT3 provided within helvella's link.
Actually, as you can see for yourself, this came to confirm that RT3 is the "mirror image" of T3 rather than refuting it, and I will not comment on the other information that he/she has also presented.
I shall stop at that and present everyone with all the best wishes for a lovely weekend.
I guess that was all I was saying. I feel good at these low numbers, which seems counter-intuitive. The title of my post had a question mark. There are certain ideas that are not as welcome here, evidently.
I am confident enough in what I have read and experienced not to be swayed by a title after a name. (Dr, MD, admin, etc)
I thought that my experience might benefit many others who have a similar issue.
I agree that the forum is very useful because of patient experiences. And there are many very helpful admins that give solid advice. The big thing I've gotten out of this forum is to make sure that your iron, B12, D, etc are all good, and that everyone has a crappy doctor/endo, which is comforting
I think what happens is that the opinions or perceived opinions of the actual medical professionals that contribute to this forum are fiercely defended.
The irony of this schoolyard fight is that it got this post into the top posts for the day and got it more exposure. Amen to that, lol...
There are several reasons/contributors for rT3 for example, stress, insulin resistance, chronic inflammation, diet, iron deficiency...
Reducing T4 and adding T3 helps to flush excess rT3 and this is supported by research and case studies; however, without treating the root cause, one might not feel well if, for example, the underlying cause is adrenal stress, auto-immunity or even both.
rT3 is also very common with Hashimoto's and Grave's and both have a strong connection with gluten. By eliminating gluten, if you have not done, you'd reduce the attack on the thyroid (the gluten molecule is similar in shape to the thyroid's cell) and reduce a great deal of the inflammation. Gluten also inhibits the absorption of core vitamins and minerals. Its undigested particles fuel bad intestinal bacteria and fungi and you'd be caught in a very vicious circle.
Kell's approach in reducing her NDT dose and adding some T3 has helped while bearing in mind that It takes a few weeks to get rid of the excess rT3 and perhaps best to wait a bit and see how you get on with the SR and then adjust the dose if you need to add T3 to the formula. I am sure kell will help by sharing her first-hand experience and learning.
There are those on this forum who will insist that rT3 is not a problem. I have read through your other posts and seen the honking of one particular individual. I saw what she said about rT3 not being your problem at fT4 levels as low as you had. I can tell you from my experience that it certainly can be.
I have reduced my NDT to 1.5 grains and am on 50mcg of T3 also. I had a TT in 2011. My muscle/joint pain and stiffness has improved greatly. My fT4 is way under range and my doc is fine with that.
Of course you can have many things going on, but reducing T4 is such a simple thing to try. It would be quite a coincidence that you went downhill after increasing levo. I do not have hashi's antibodies and I'm not sure where my bad conversion comes from. I have endeavored to make sure B12, D, iron, etc is where it should be. Sometimes you just aren't going to be able to address the root cause.
There have been a number of go-rounds on here about rT3, but here is an exchange between myself and Dr. John Midgely (Diogenes) regarding Rudolf Hoermann's response to Finnish endocrinologists. These men are both advisors to this forum. Let their words ring in your ears instead of the incessant honking of 'rT3 doesn't do anything'!
So then the statement this statement is attributable to Rudolf Hoermann? Is this his current thinking?
Reverse T3 is not an inactive metabolite as has long been thought, rather it acts as a T3 blocker. Our whole view on the non-classical hormones has dramatically changed in recent years and new roles are emerging (Hoermann et al. 2015).
diogenes
diogenesin reply to Kell-E
Yes I think so, but exactly how rT3 interferes is still up in the air. It isn't at the receptor level so must be in the biochemistry of T4-T3 conversion somewhere.
Kell-E
Kell-Ein reply to diogenes
But the idea that rT3 does interfere with T3 is not up in the air...it is just a matter of how it interferes? Some on the forum feel that the advisors to this forum have declared that rT3 is utterly inert. Evidently that is not the case.
diogenes
diogenesin reply to Kell-E
Well I never said that. I've said that rT3 seems to have some effect but no one knows exactly what. I simpy debunked the receptor competition idea as an explanation.
Kell-E
Kell-Ein reply to diogenes
I know that neither you nor your colleagues have ever said that. Some have run with the receptor concept, drawing the conclusion that rT3 is inert. Just because it does not interfere via a particular mechanism does not mean is does not interfere. I'm glad to see this in print, thank you!
Kell-E
Kell-Ein reply to diogenes
Is the study from 1982 the one that proves that interference is not at the receptor level?
rT3 interferes with T3 but it also inhibits T4 to T3 conversion. So it is extremely effective at lowering metabolism.
Another 5 days w/o levo would put you at about 25% of levo remaining. Another week and 12.5% and every extra week half of the week before.
I would say it is possible to overcome a poor T3/rT3 ratio on NDT if conversion is adequate. Or at higher doses of NDT you max out poor conversion (it can never reach 100% conversion to rT3 from T4) and overcome rT3 that way. That's what my new GP does with his patients. This results in large doses of NDT and over range fT3. Your doctor is not likely willing to do this.
So, if you find that your dose of NDT that you are allowed by your doctor is not resolving your symptoms, you have several choices. Source your own T3 and secretly take it. It has a very short half-life and if you don't take it for a few days your blood tests won't show it. Plus you have Hashis so you can always pass it off as a flare, lol.
Or you can source your own NDT and find a dose that works for you.
Don't stay unwell just to keep a doctor happy. It is your body. We are not school children. Having said that, I do understand your concern...but I'd say it again!
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")