I'm a GCA patient, having been diagnosed in AUG 2022. I started on 60 MG, and have weaned down to 12.5 MG at present. Forgive me for being "anal," but I'm an engineer and tend to think in terms of graphs, charts, etc. I thought I'd share the following graphs -- for 2 reasons. First, please correct me if I seem to have misunderstood all of this Secondly, it might be food for thought for others who have either GCA or PMR.
I'm attaching 4 graphs above. I know they are hard to read, but if you can see the numbers then try to follow my reasoning:
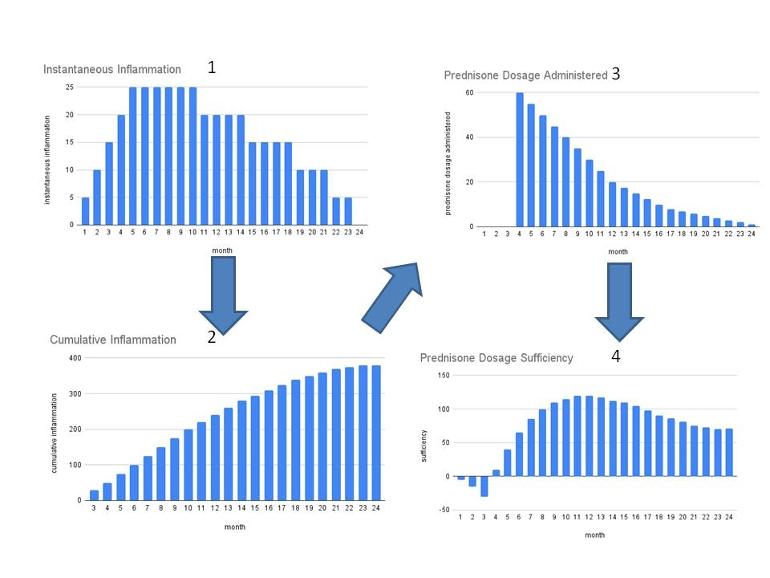
Graph #1: My "theoretical" instantaneous inflammatory response (in terms of equivalent prednisone levels). As you can see, I'm assuming I had a 5 MG inflammatory response the first week of my disease. At this point, I didn't even know I had the disease. The 2nd month, I had a 10 MG inflammatory response. the 3rd month, I had a 15 MG response, and so on. I have no idea if these were my real numbers. All of this is theoretical.
Graph #2: The CUMULATIVE inflammation my body had experienced. As you can see, by week #4, I had experienced an equivalent of 100 MG of inflammation. At this point, according to my "theory." I started having symptoms.
Graph #3: This is a chart showing my actual prednisone dosage that had been administered. As you can see, I started at 60 MG for a month, then 55, then 50, etc.
Graph #4: This chart is the DIFFERENCE between the accumulated inflammation and the administered dosage. If the DIFFERENCE is negative, the dosage is insufficient. If positive, the dose either matches or exceeds the inflammation.
If these graphs represent "the way things work," then they suggest that if I am having symptoms at say, 16 months into my disease, then 1) my instantaneous inflammatory levels are/were higher than I thought or 2) the prednisone dosage administered was not high enough.
This also points to a need for us to know our "instantaneous" inflammation levels. As I understand, ESR and CRP are the only current measures of inflammation -- and at least for me, these 2 indicators are weak indicators.
Thanks for your patience in reading all this.
Written by
montebello
To view profiles and participate in discussions please or .
I think what is most important is how do you feel and your symptoms or lack of them. CRP and ESR may measure inflammation, but many things can cause these to vary. What you really need to know if changing your diet for example changes things or taking certain exercises and plotting how you feel against trying various changes to how you live with GCA. Having dosage included is a good idea of course.
Thank you piglet. I understand what you're saying. But what I'm really trying to understand is the relationship between the inflammation that my body is producing and the prednisone I am taking to combat it. I'm not trying to feel better right now (although I'd love to!) -- I'm merely trying to understand the disease a bit better -- SPECIFICALLY the relationship between the inflammation my body is producing and the prednisone I am taking to combat it.
In thinking about what you've said, I suppose that if diet or exercise changes affect my symptoms, then they must also be affecting the inflammation levels within my body.
It is a bit bewildering to me that someone, somewhere has not found a way to measure the amount of inflammation being generated by this disease (because as you said CRP and ESR can be affected by things other than GCA or PMR).
I have ridiculously high ESR and CRP. No doctor can tell me why although I would love to know. My CRP is usually eight times the top of the normal level and ESR double to treble. This is why I would not use your inflammation levels against your steroid dose to try and extricate any sensible result.
I feel fine. When I go over 100 the GP does phone up and checks urine etc. They have checked for cancer, heart disease etc etc and given up. They have decided it is just me. I have a very low temperature and also low blood pressure. My brother reckons that I was meant to live on another planet.
You can assess it either on the basis of blood tests though the inflammation markers are non-specific or you can do PET-CT at the outset to assess inflammation points in PMR, it is less useful for GCA. But the level of the markers isn't actually representative of the severity, some patients don't mount that response at all and a very high ESR/CRP doesn't mean you need more pred either in practice although some doctors will give a PMR patient far too high a dose because their marker was high.
But you seem to be looking for an ongoing monitor - and PET-CT is not an option there as the radiation load and cost are too high for repeated use. And that is where the empirical approach of titration of the dose comes in. I may be nuts in your opinion but I do understand that medicine is as much an art as a science and while it has parallels to engineering, it doesn't obey rules,
PMRPro, I hope you've read my response to koalajane. I most certainly do not think you're nuts! Far from it! I was merely expressing my exasperation about myself for not being able to communicate more clearly. Sorry if you thought otherwise if even for one minute.
I had, I read all the replies, Just a sllight reminder that this is an international forum with several versions of the English language being used - care is required
The most reliable indication of the inflammation being controlled is symptoms.
I may have totally misunderstood but are you thinking in terms of the pred having cured the source of the inflammation? Pred cures nothing - the inflammation is due to an autoimmune disirder that causes the immune system to attack body tissues, causing damage and symptoms. This is ongoing for an undetermined time and there is no way of stopping it, but for most people it does burn out eventually and then you need no pred. In the meantime, the initial dose of pred is to clear out the accumulated inflammation and is generally a high dose in GCA to reduce the swelling due to the inflammation as quickly as possible and reduce the risk of sight loss which is the most dreaded complication of GCA - when it is gone, it is irreversible. Having achieved that, the idea is to reduced the dose of pred to the lowest level that manages the daily batch of new inflammation created in the early morning. This process is also called titration - and just as in chemistry you reduce the dose until you just overshoot and then go back to the last dose that worked well. You are looking for the lowest dose that just does the job.
Unfortunately, bodies don't work like machines ...
So if I am understanding a bit of what you said about GCA, if you have no inflammation but have some head discomfort you dont need to take prednisone? I am confused....
No - I didn't say that I hope. You need enough pred to keep you free of symptoms and that should also make the blood markers they use low as well. But some people never have raised markers and they also lag behind an increase in inflammation. However - not all headache is GCA - it can be due to all the things you'd assume if you didn't have GCA, plus reducing the dose and once you get to adrenal territory it could be adrenal insufficiency. It is a complicated thing - you have to know YOUR GCA, YOUR response to pred and how changes in dose affect you.
not sure if understand the difference between cumulative inflammation and actually administered dose shown in Fig 4 (if I interpret your description correctly) - wouldn’t it be rather the actual inflammation the pred dose needs to be matched to to obtain a dosage sufficiency? I agree that there might be an inflammation legacy effect in a way that the longer the inflammation lasts the higher the dose needed to see an effect; but I‘d rather think that this would be also mirrored by the actual inflammation intensity . But maybe I just didn’t get your point.
THANK YOU DeepThought2! Your response is exactly why I posted this message. I was hoping that someone would take the time to understand what I was trying to say, which you clearly have done. Again, thank you!
In thinking about what you said, you make a lot of sense. It's the inflammation intensity that matters -- not the cumulative inflammation as I have plotted. Saying it differently, it's the inflammation intensity that must be countered by the prednisone, not the cumulative inflammation.
But maybe inflammation intensity is directly related to cumulative inflammation, no? That is, if my body produces, say, the equivalent of 5 MG of inflammatory substances per day -- unchecked by any oral prednisone for, say, 30 days, then my body would have "accumulated" the equivalent of 150 MG of inflammatory substances. These "unchecked" substances would certainly lead to the "inflammation intensity" that you are suggesting, no?
I agree that there is a legacy effect and cumulative inflammation and inflammation signaling will certainly lead to higher actual inflammation responses - especially the interleukin signaling can prime more systemic responses to local inflammation and thus can cause a positive feedback loop. Concerning markers for inflammation - that is a tricky point and I think symptoms you notice are important but could also be misleading (side effects of medication, symptoms related to pred tapering etc). So it stays a trial and error thing. There is a rather experimental marker (calprotectin in blood serum) . Calprotectin is released by granulocytes and is seen as a proxy for local inflammation levels ( and might give indication on disease activity also under medication - pred but especially Actemra).
I agree - it is non specific for localized inflammation - the main advantage is rather that it gives indication if there is still an inflammation when systemic proinflammatory pathways are blocked by pred or Actemra
As I said, it is still experimental. There are a few studies related to Vasculitis (the second and third link also includes GCA). My rheumatologist at Uni Freiburg is involved in a study on calprotectin, GCA, residual disease activity (PET-CT) and relapse probability and says the preliminary results look convincing especially for the use under IL-6 inhibition. But it is not published, yet. So I get it measured regularly (as part of another study) and it is low at present 😀
Yes, DeepThough2, that's the problem I'm having with relying on symptoms -- heck, many of the symptoms of GCA are also side effects of prednisone!! It's encouraging to know that there are those who are pursuing other markers (aside from CRP and ESR). Thanks again.
Thank you for generating an interesting dicussion, Montebello. It would be so helpful to know the answers to all the points made but I think the only way this will happen is when there is a biochemical way of identifying inflammation levels similar to diabetes for instance. Obviously this would be immesurably helpful for a burn out illness like ours. Perhaps AI will bring this about, or the end of everything, whichever sooner.
To further complicate this I believe there is cumulative inflammation and also what can be called 'escape' inflammation. The cumulative inflammation builds up to the point where bucket is full and discomfort so bad that we need to increase pred.
Escape inflammation is where there is inflammation left over from the pred but it does not build up - leads to ongoing low level symptoms but no need to increase pred and hopefully will get better in time and can start taper again (or gets worse and can't).
In my view, the best way to manage GCA and PMR is to develop interoceptive/somatic awareness to try and distinguish the illness from impact of pred (as you say it can result in similar symptoms) any other external or health factors, and then the impact of adrenals - the ultimate complicating factor at lower levels. May be possible/interesting to attempt this diagrammatically...
Thanks for the response. There's a point I'm not sure I understand:
"Escape inflammation is where there is inflammation left over from the pred but it does not build up - leads to ongoing low level symptoms but no need to increase pred and hopefully will get better in time and can start taper again (or gets worse and can't)."
How can there be left-over inflammation (after prednisone) that does not build up? Where would it go? How would it be accounted for?
BTW, I laughed when I read your comment about AI. Either the solution to everything or end of everything.
I can't answer your questions properly, wish I could, but this is what I mean.
Around 6 months into GCA on around 17.5mg following some wobbles I went to a well respected UK rheumy. I was getting ongoing but intermittent head symptoms - sore spots, low level stabs, twinges and tingles. I assumed I needed more pred but he said it was 'escape GCA' and to ignore it unless it got worse. This was a big relief to me. I ignored it and each month of tapering I would get similar symptoms but they got less rather than worse.
I asked him what he meant by escape GCA but he didn't explain further. Hence my explanation that each day there is a bit of left over inflammation but not enough to build up and cause problems. Over time, if the GCA is not highly active it gets less.
Now I have PMR and I notice a similar thing.
Hence my point about being familiar with inner sensations so we can try and differentiate what's going on.
I had a flare after third vaccine and it was different from escape GCA by being stronger and more persistent - active rather than grumbly.
Oh-oh. I didn't mean to imply that either you or PMRPro were nuts! I live in the US, and "nuts" is like saying "drat," or "heck," or "darn it," or things like that. It's more an expression of frustration in oneself as opposed to belittling someone else.
I was frustrated with myself that I was not more clear in my post.
I'm wondering if all this deconstruction is helpful. It is more complicated than your graphs. There are surges in inflammation on a daily basis and there can be accumulated inflammation. Just take the drugs you need to control the condition on a daily basis. This is the time to be pragmatic.
Hi there! I should be in bed, but I had to answer you. That was fascinating from an analytical point of view--the catch is that the disease is unpredictable. I lost sight on August 5, 2019, and was started on 125mg Pred and then in October Actemra plus 80 milligrams of methylprednisolone ( stronger than Pred) each day, the injection weekly. I just got to 10 mg plus Actemra in February 2023. Plus, while on Actemra, your ESR and CRP are always normal, so it is symptom treatment only, the best kind in my book.
As I looked at the charts...if you look at Chart #2 and #3, flip #2 upside down and over...it would fit perfectly onto #3 like a puzzle piece. It looks as though your inflammation has a direct correlation to the amount of prednisone you are taking. Have you ever talked to your rheumatologist about Actemra since you are in the States like I am? Gosh, I was on it not long after it was approved. Maybe it would help you too.
Just one other thing to share; because of my symptoms these past three years, my pattern ran something like this~~per day, 80,40,60,40,15,40 last fall, and when I got to 10mg this year, I've cut by .5 mg per month and sometimes held for longer depending on my symptoms or sense of well-being, all the time on Actemra injections. I'm at 3 mg daily now and holding until I start and end some travel. Even now, I usually have a headache each day and take a few Tylenol, and it is gone. The day Tylenol doesn't cure it, I'll be concerned.
Please take it slow and take care of your eyes.💞
PS That chart is exactly what my husband would do, then put it in a plastic container and label it. I'm surprised I'm not in a containerand labeled~!! 😂😅
Grammy, you are so funny! Are you sure you have not been labelled and put into a jar (ha)!
I've been heeding your advise ever since I've "met" you. But to be honest, if I were to rely totally on "symptoms," I might still be at 40 MG PRED per day. The most serious symptom I continue to have relates to my vision. The day after I started at 60 MG, my vision was cloudy and blurry. It's never gotten better. Also, I've been experiencing double vision (when I tilt my head in either direction) since before I was diagnosed. At the last visit I had to the ophthalmologist, I asked to be referred to a neuro ophthalmologist (at your suggestion). I'm awaiting an appointment.
In the meantime, I get "pleasure" exploring my understanding of things -- which is why I initiated this post. Thanks, as always, for your positive comments.
Montebello...we are friends, right?? You just said, "The most serious symptom I continue to have relates to my vision." Think about that! It is true we get some blurriness from the prednisone; I've not heard of double vision. I experienced some blurriness for sure...but please don't let blindness be your next symptom.
I didn't know what GCA was till then....only then. You are an intelligent man. It took you six years to get off prednisone with PMR. Even those who suffer every day from PMR will tell you they would rather have that than GCA. Your inflammation markers can be 'decent' or perfectly normal, and you could still be in trouble with your GCA.
One more thing and then I will leave you in peace...you said, " But to be honest, if I were to rely totally on "symptoms," I might still be at 40 MG PRED per day. " Truer words could not be spoken~~and that would be because you needed it. That is why it has taken me three years to get down to 3mg I don't regret it...I can see out of my right eye....Who wants to be a one-eyed champion? Only you may not be so lucky if it picks up a full head of steam and will not quiet down; that is what happened to me.
You know I wish you well, you know I am concerned but I won't nag at you. Please take care.💞
PS I assume you see a rheumatologist and not an MD only or ophthalmologist only; strictly my personal opinion 😉
FYI, I saw the rheumy today. He totally dismissed my double-vision issue, probably because I've been telling him about it since AUG22. In fact, he told me it's time to decrease my dosage to 10 MG (from 12.5).
He also told me he expects my double vision to "go away" eventually. To be honest, I'm beginning to think I know more about this double-vision issue than he does. All I've read about double vision is that it typically resolves itself within days of taking prednisone, and if not, it's probably permanent.
Vision issues -as my reply to Grammy80 - and I agree with her, you do need to take more notice of symptoms -once sight loss is gone, it’s gone. As we can both testify.
Sorry but my feeble brain doesn’t understand your units of measurement in your y axes. Why do you measure inflammation in mg? Or do you mean your inflammation must have a direct equivalence to your dose and that can be used instead of CRP/ESR?
SnazzyD, yeah I know the units I use for the y-axis is confusing. I use "equivalent MG of prednisone" because I don't know what other units to use. It'd be like using "tablespoons of sugar" instead of "calories" if there were no such unit as a "calorie." I hope this is a bit clearer.
Like you, I am happy to think in graphs (polymer scientist, with degrees in chemistry, mathematics and materials science). But I think physiology and disease can be difficult to understand in those terms because (amongst other hypotheses):
1) The inflammatory agents (cytokines) are not released at a constant rate, but their concentration tends to peak in the early morning.
2) The body is not a closed system. The 'instantaneous inflammation' may be affected by other stimuli (other infections, previously damaged components of the immune system and additional stress), so may not be generated at a constant rate.
3) The effect of the corticosteroid may not be linear. It is not efficacious by just being in the gut; it has to be absorbed into the blood; thus, diet might affect its uptake.
4) Then, your prednisone has to be converted to prednisolone (by reduction of a keto group), which is the active corticosteroid.
5) A fraction of the absorbed dose enters cells to bind with corticoid receptors, in order to suppress the inflammation.
6) At the same time, the drug will be eliminated from the body. (Prednisolone has a half-life of around 2-3 hours in the blood, but will persist longer if bound to a corticoid receptor.)
So, there are at least four steps in this reaction sequence - plus the competing 'elimination' processes.
The symptoms themselves are a realistic - if somewhat subjective - measure of the disease. ESR and CRP might appear more objective, but are only measures of inflammatory response, so can be affected by other things. They also require blood sampling, which generally (outside a clinical trial) only occurs sporadically.
I have found simple temperature measurements can be quite enlightening, as more frequent indicators of inflammation - and give me endless fun putting them into a spreadsheet. Although, like CRP and ESR, are affected by other things, so a degree of circumspection and interpretation is required.
PRL1957, wow -- a fantastic response with so much to think about. I've included my thoughts below:
1) The inflammatory agents (cytokines) are not released at a constant rate, but their concentration tends to peak in the early morning. Yes, but they can imaginatively "summed" each day and then "imaginatively" plotted, which is what I've tried to do in Graph #1.
2) The body is not a closed system. The 'instantaneous inflammation' may be affected by other stimuli (other infections, previously damaged components of the immune system and additional stress), so may not be generated at a constant rate. Yes, but are the "inflammations" you mentioned of the same nature as the GCA-related inflammations? I know it's hard to follow me, but the Graphs are "theoretical" in nature and assume that the inflammations I've plotted are specific to GCA.
3) The effect of the corticosteroid may not be linear. It is not efficacious by just being in the gut; it has to be absorbed into the blood; thus, diet might affect its uptake. This is a very interesting comment -- at least to me. If diet is a factor in corticosteroid efficacy, the medical community (at least where I am) has done a horrible job in communicating this. I know I have to watch out for diabetes while on PRED, etc., but no-one ever told me what kind of diet to be on to maximize the effectiveness of my daily prednisone.
4) Then, your prednisone has to be converted to prednisolone (by reduction of a keto group), which is the active corticosteroid. I have learned, on this forum, that Europeans are prescribed prednisolone, while those of us in the US (and Canada) are usually prescribed Prednisone. I've always wondered what is the difference, and now I know. I wonder why we're not prescribed prednisolone here in the US?
The symptoms themselves are a realistic - if somewhat subjective - measure of the disease. As I've replied in another post, it's unfortunate that many of the symptoms of GCA and side effects of prednisone are similar -- which makes depending on symptoms alone ineffective.
I have found simple temperature measurements can be quite enlightening, as more frequent indicators of inflammation - and give me endless fun putting them into a spreadsheet. Really!? I had no idea! Could you say more? Daily readings? What kind of thermometer?
Another engineer here, and I’ve applied mathematical analysis to most problems that occurred throughout my experiences. When PMRGCA struck me, I set up my spreadsheets and graphical interruptions but incorporated an objective numerical representation of the pain of the various symptoms I felt morning and evening. However, the only correlation I discovered was between the Pred and insulin I needed, and that titration I have under control, although there is a number variations that I have to take into account for effective calculation.
The advice given in this forum has been far more useful and I doubt I could apply any mathematics that would explain it. I can only concur there are greater mysteries than can be explained by math and physics (yet) and the insight of fellow sufferers is a veritable goldmine of useful information.
However, don’t give up quietly and keep the spreadsheet alive!
JaiSea, I am on this forum daily and read almost all the messages and TOTALLY agree with you regarding the advice and guidance of the folks on this forum. They got me through PMR in the past and are getting me through GCA at present. I thank God for this forum, and the people on it.
While I will say that clearly your charts are a good distraction for you in terms of how you think as an engineer. As a human, I'm not understanding them or unable to read them and not sure you're incorporating all the "facts" that influence the data you've plotted. If you're a watcher of X-files: "Just the facts Scully/Mulder, just the facts."
"I am taking to combat it. I'm not trying to feel better right now (although I'd love to!)". Why combat it? Why not want to feel better? This is a very stealthy enemy you're trying to "combat". There are so many factors, such as diet (low carb), exercise (a little), illnesses (this is an autoimmune disease), which influence the inflammatory markers. It's not all about the numbers (CPR, ESR) but they are what we have to use. I also think that by now there should have been other means of measuring inflammation, but in many cases especially with PMR, these diseases are not taken at their full potential, i.e. "not as seriously".
You've done remarkably well at tapering, but how are your symptoms at 12.5 mg? If you are on too low a dose, the inflammation will build up like drops in a bucket, until you have a flare and then boom you're almost back to square one. Therefore, how you are feeling at this dose (particularly painwise) is very important. Why drop 5 mg. if you're in agony?
I've had PMR since before Jan. 2022 although I didn't know I had it until then. It's been quite the roller coaster ride, but I've learned to accept it, not combat (or even understand) it, because one cannot. It's a new ballgame daily pretty much. My attitude is a positive one, but I do get discouraged occasionally. There are good days (most times) and better days.
Quality of Life is something which must be considered in your tapering plan. We do not have to live daily in constant pain from inflammation, as the pred is meant to control it. We are not trying to reduce relentlessly to zero pred. The lowest dose which controls the pain is the one we should be "aiming" for. All the best to you and I hope you receive the answers you're looking for in our forum. In any case, stick with us. Cheers!
I need to be more careful in the words that I choose. I should not have said "combat it." I should have said "control it." I'm totally with you, understand you, and agree with almost all that you said. The only point of disagreement is in the need FOR ME to try to understand more about it. Understanding is a key to life. Understanding one-another, understanding the mechanisms of life -- or at least trying. But "beauty is in the eyes of the beholder," so if that's not your thing then that's fine!
As for my symptoms, I'm doing the best I can. I've been though PMR myself and totally understand the dangers of decreasing PRED dosages too fast. On the other hand, when I look at my skin, or consider the condition of my GI tract, or continue to have increased pressure inside my eyes, and and on and on, then just like all of us I try to balance as best I can.
Nagswoman, I know it's hard to understand my approach or reasoning, but I've tried to quantify the inflammatory issues by using the phrase "equivalent mgs of prednisone" simply because there seems to be no standard "units" that are used to talk about inflammation. An analogy would be for people to talk in terms of "tablespoons of sugar" instead of "calories" if there were no such thing as units of calories. I hope this makes sense.
I see your angle - but there are a lot of variables that affect the dose each individual requires and it can also vary for an individual over time. That is why the high dose followed by a titration is use to identify the dose that each patient requires. Even taking it on a full or empty stomach and what the food was makes a difference.
Not sure that the spike protein has nothing to do with all this. There are plenty of us who were diagnosed during the "age of covid," and have questioned just what triggered it all. PMR itself is a pretty broad label of patients who all have both similar and unique symptoms and respond differently to treatment.
There is no single cause of PMR and several vaccines can trigger the immune system to develop an autoimmune disorder, not just PMR. But so can the illnesses that they are to protect you against, or other illnesses or anything that stresses the immune system (that is in a biological sense). Covid and the covid vaccine is in that sense just another in a long list of potential triggers.
I don't think the SARS-Cov2 spike protein has adversely affected me. I had covid during February, this year, and it felt like a mild cold. (We only know it was covid because my wife had it too, with more severe, classic symptoms.)
In my case, I suspect the trigger for my PMR was the single strand modified viral RNA in the (Pfizer -BioNTech) vaccine, which can 'upset' the immune system, e.g. see Vierbuchen et al, Allergy. 2019;74:223–235, DOI 10.1111/all.13680
But, if so, I do wonder how I was able to deal so easily with covid itself, including spike protein and viral RNA.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")