Current dose 50mcg . Have had to reduce because of elevated liver enzymes. HCT is currently 37 but it does fluctuate. I haven’t had to have a phlebotomy in months. I wouldn’t say everything is exactly stable. Im better than I was before I started taking it though.
Barbiebreath, I was at 250/300 mcg Besremi when my liver enzymes skyrocketed, so I'm off it for now. A month later they were even higher. I'll be tested again this week. How long did it take your enzymes to normalize after adjusting dose? (If I go back to Besremi I'll probably ask for much lower dose, even if some current studies say use higher.) After 6 doses (increasing from 50 to 300) my HCT was down to 43.3 and platelets to 402. (Had never been so low in three decades...) I'll update this answer after testing this next week, but since I'm not actively on Besremi right now, perhaps I'm not fodder for the survey, EPguy. Also, I was just getting into the groove when I had to stop, so no stability reached.
Update: Recent blood test after a 6 week holiday from Besremi (which is looking permanent according to local oncologist) showed HCT was within norms, Platelets on the rise after getting almost to 400 after 12 weeks of Besremi, and liver enzymes still very high despite two weeks of liver detox meds from acupuncturist. Thanks for added liver peptalks, below, I'll keep trying to clean up the beleaguered organ. I made another video appt at the Mayo clinic, as I've the distinct impression my local doctor and the clinic itself have way too little experience with MPNs. I'd more than a little demoralized and feel trapped close to home, as the doctor even discourages a plane trip to see my sister due to PV and clots. Medicare still saying they won't pay for 6 week$ of expensive Besremi injections. Clinic is filing challenges at this point.
I agree on keeping doses lowest possible, the info so far here, and last year, points to this as good practice for many. If you cannot return to IFN, Rux is an option, a quite good one from the recent data. That is where I am now.
Pegasys interferon alfa-2a is an alternative to Besremi interferon alfa-2b and less likely to spike liver enzymes (see brief video below). Many doctors appear to be failing to tell their Besremi intolerant patients they may find Pegasys agreeable and thus potentially gain the multi-decade long disease progression slowing or stopping survival benefits of interferon-alfa (something not documented with Jakafi): youtu.be/DzRroOp7JTE
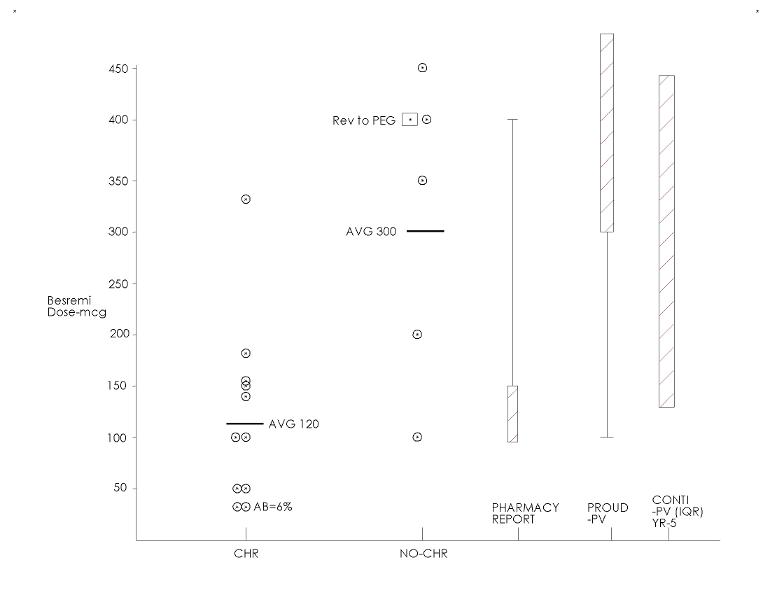
We discussed this one recently. His observation relates to the dose conversion, ie BES is too high compared to the common doses of PEG. He did say "due to the drug" at the end but the preceding dose comment seems to be the context.
This is right on the point of the post here and last year, effective doses in our own group are apparently much lower than the trials used.
My severe vax reaction may well have not happened if I'd been on the lowest effective dose.
Re Jakafi, the disease modification ability has recently been explicitly documented, (allele reduction vs progression was an endpoint to the study) This separate subject and its positive implications for IFN are addressed in other recent threads.
Hydroxyurea has disease modification ability too - during the first 2-3 years whereas interferon has a multi-decade long track record. We don't know if Jakafi might have long term disease modification ability too as it's only been on the market for about 11 years.
We do know the subset of Jakafi users that attains allele burden reductions are not able routinely lower their dose and/or frequency of dosing as a substantial subset of interferon users are able or take complete vacations from the drug for periods of 1-4 years while maintaining their normalized blood counts. So unlike interferon, Jakafi is never referred to as a drug capable of "operationally curing" a subset of MPN patients or inducing a durable state of "Minimal Residual Disease".
In 2021, after 9 years experience with Jakafi, Dr. Silver said: "I don't think the Jak2 inhibitors are going to change the basic biology of the disease." youtu.be/QdEoPlcuf6A
we discussed this before , what was known and said about Jakafi in 2021 ie at time of this vid is somewhat out of date, the important papers on Rux reducing allele etc are just out recently.
I love that phrase “operationally curing”, at least it confirms it’s a subset., is the patient cured or not, (they are not cured unfortunately) they can’t be just “operationally cured”. That’s sound like being a bit pregnant.
As ainslie notes, you have offered this info elsewhere and we've covered all of it well. It is not the subject of this post but I feel a need to provide my take.
--
I have also posted in detail the considerable benefits of IFN and Dr Silver's pioneering work with it. But there are voice members who cannot tolerate IFN, and others who prefer the risk trade off of other therapies. Pointing to the deficiencies of the alternatives is not helpful for these members. As one of them, and in considerable distress, we need messages of hope not despair. Please offer the favor of evaluating the details here:
--
On Rux it so happens that my switch to it coincides with very recent reports that are dramatically changing the view of Rux for PV. From some of my recent posts:
--
Molecular response: In this image (left) from Majic PV Rux trial the % with deep MR is large. This is the sort of result we see with IFN, and was not known at the 2021 date of Dr Silver's comment. In the right image the result meets any common definition of disease modification. In fact this prospective data does not exist for IFN, while it supports the assumption that IFN shares this benefit, ie molecular response modifies disease, and getting to less than 2% stopped progression on this trial.
Best molecular response: In the same study the right image is from, Rux provided 6.5% of pts with undetectable VAF. In the Ropeg trial, this criteria is similar at 5.4%. (this is in a supplement to the Ropeg study) These are from different studies and may not fully comparable, but it's clear only recently that both IFN and Rux are both impressive in ability to wipe the mutation. Can Rux be stopped in these cases? I don't think it's been tried.
Handicap: The Rux trials have been handicapped by requiring any HU pts be intolerant to HU. The Ropeg trial allowed only HU tolerant pts which might bias to a better result. We might find even better results for Rux in the RuxoBeat trial without this handicap.
HU: It is true that no study has shown disease modification for HU, but it can for many offer positive life modification.
MPL: One of studies had a pt with MPL reduced to undetectable. So Rux may be worth considering for MPL ET
--
In sum: Both IFN and Rux seem to be capable of similar deep benefits in PV as documented only very recently.
I'm not aware of any of Jakafi's long standing fans in the USA - like the MPN specialists at MD Anderson, Sloan-Kettering, Mt. Sinai, John Hopkins, Stanford, Cleveland Clinic, etc., coming out and making PUBLIC statements to the effect that they now consider Jakafi as a drug that appears to have disease modifying capabilities comparable to interferon.
Just today a Patient Power video came out on the topic of disease progression risk in polycythemia vera where Dr. Gerds at Cleveland Clinic made no mention of Jakafi as being a drug a PV patient should consider if their goal is to reduce the chances of progression:
that’s because it’s new info, the paper by Clair Harrison is new, I know for a fact Mount Sinai know what Rux does as one of their experts told me at the recent MPN Phoenix conference at Mayo, ditto with Dr Kiladjian at same conference. So it will become more PUBLIC soon.
this is misleading, it’s only a very small minority that can have Peg or Bes holidays, everyone knows that, I wish it was more but it simply isn’t. Still possibly the best drug for PV/ ET but we have to be realistic
»The majority of ropeginterferon alfa-2b-treated patients (54.3%) achieved a JAK2V617F allele burden <10% at 5 years and might be potential candidates for treatment discontinuation ».
what it actually says is 30.4% might be considered for treatment discontinuation according to previous findings. However prerequisites for treatment stop remain a subject for research. I will also add that the 30.4% is taken from those who didn’t drop out which at 6 years is around 50-60%. Interestingly in this paper it states complete haematological control ie all counts in range was only achieved in approx 50%. It’s a good drug but we have to be realistic what it can and can’t do as per all drugs
You wrote: « what it actually says is 30.4% might be considered for treatment discontinuation »… »it’s only a very small minority that can have Peg or Bes holidays, everyone knows that… ».
In my opinion, 30% can’t be considered as a « very small minority ».
7-14 years ago Dr. Kiladjian conducted a 72 month long PVN1 study where newly diagnosed PV patients were given Pegasys interferon as a first line treatment.
38% were able to take Pegasys holidays and 81% of those still had normalized blood counts 3 years later so did not yet need to restart Pegasys.
Another 30% continued taking the weekly injections, 27% discontinued for toxicity, 5% dropped out for non-toxicity related reasons.
So far, none of the MPN specialists that have worked with Jakafi over the past 11 years has reported that a subset of their PV patients were able to take vacations from the drug after achieving normalized blood counts. youtu.be/vuhwGEi4Y_k
He said higher doses correlate to better MR. Seems intuitive, but the more recent Ropeg study (this video is ~6 years old) noted no relation to dose.
CHR and MR are related. This matches recent studies as discussed before, implying min dose required for CHR is best.
At 9:13 he noted the autoimmunity risk. I can say personally this is real, and is one of the adverse events among our treatments that can be permanent.
please do liver cleansing, stop any alcohol and reduce all additives from foods. There are so many ways to help the liver! Keep your liver as clean as possible and functioning well. There’s so much info in internet on this subject. Do it naturally and take natural supplements for support! The liver is an amazing organ that can repair itself fast, unless it is too damaged, but don’t wait for it to clean and save itself if it’s been overburdened. 🙂
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.