Good news from the most recent CBC. HCT back down to 43.8.
As my iron levels continue to improve, erythropoiesis is naturally also increasing. HCT = 46.0 on 03/25. It was down to 44.4 on 04/11. However, the trend line is up over the last several months. The MPN Specialist does not want to increase the Besremi dose significantly due to the ongoing issues with lymphopenia and neutrophils hovering above and below reference range. The leukopenia is a concern for me as well. I am also concerned about the possibility of needing another phlebotomy as I feel so much better with my iron levels higher. My goal is to manage the PV without using phlebotomies.
I proposed to my care team that we bump the Besremi dose up to 110mcg. Really just using the top of the plunger to measure rather than the straight line lower on the plunger. In the absence of objection from my care team, I did up the dose on 04/13. Note that this level of a dose increase would be expected to have minimal impact from a purely dosing perspective compared to the recommended dose increases of 50mcg. I figured at least it was an action I could take with minimal risk that maybe would help. If nothing else, perhaps just create a Hawthorn Plant effect. Perhaps just a bit of mind over matter.
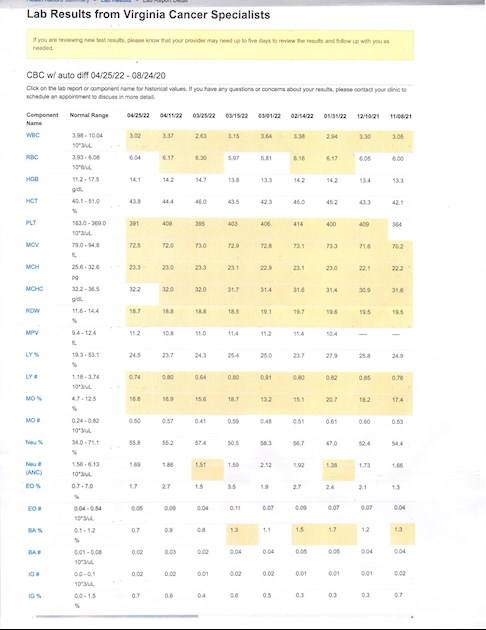
Highlights from the 04/25 CBC
HCT = 43.8 (below target)
PLT = 391 (below target)
LYMPH = 0.74 (mild lymphopenia)
NEUT = 1.69 (low normal)
WBC = 3.02 (mild leukopenia)
In short, all numbers moving in the right direction with acceptable side effects. Also note that since I have started taking Claritin daily, the itching/pop-up rashes have stopped.
I just met with my wonderful local hematologist about the ongoing treatment and continue ongoing consultation with the MPN Specialist. My plan at this point is to continue with the 110mcg dose of Besremi. If the HCT continues to creep up above 45%, then my plan is to bump the Besremi dose up to 125mcg and closely monitor my response. I will work in close collaboration with my MPN care team on this plan as needed. Hopefully no further dose increases will be needed. We did discuss having a single phlebotomy as an option, but I would prefer to try a Besremi dose increase first.
I relayed all of the above to the Biologics (specialty pharmacy) nurse who calls on a regular basis to see how I am doing. The nurse was very surprised to hear about the atypical dosing level. I explained the rationale and related what was going on with the Besremi efficacy/side effects. I usually get a follow-up call from PharmaEssentia when there is something new to report. We will see what they say when I update them. I always remind them that we need smaller syringes with better dose titration at lower doses. I hope we will see that sooner rather than later.
All the best to all of you all.
Written by
hunter5582
To view profiles and participate in discussions please or .
I was on 45mcg of Pegasys. It was controlling the erythrocytosis; however right before I switched to Besremi, my HCT popped up to 45.2%. That is why I decided to up the initial dose from the recommended conversion dose of 63mcg to 100mcg. What is going on is that my iron levels are increasing, which is driving up the erythropoiesis. The besremi is working, but has to still control the excess production of RBCs in the presence of higher iron levels.
Correct. With a little dose titration as needed. It is expected for erythrocytosis to to increase as iron levels increase. Itis the flip side of why phlebotomy is used to treat PV. Less iron = less RBCs. More iron = more RBCs. Unless something else (Besremi) prevents it.
Sometimes I would like to raise a question about the 45 or below HCT guidance for PV. If a patient has normal or near normal readings on many of the important CBC data/parameters, should the 45 or lower HCT be "strictly" followed; or just follow the normal range based on the laboratory standards that is higher (50 HCT from the lab that I go to).
I thought that the purpose of observing 45 or below HCT is for preventing cardio complications (stroke and heart attack); and if the PLT is elevated then prevent the potential of blot clot. So, if a patient who have demonstrated near normal or normal results on CBC for a few months; wouldn't it be acceptable to follow the usual HCT range and then avoid (frequent) phlebotomy?
Sorry for this idea which is a deviation from the usual medical or WHO guidance.
My understanding is MPN makes patients uniquely sensitive to HCT level, and this discovery and the subsequent tight control of HCT has provided a good part of the improved event free survival seen over the last 30 years.
<<Managing Hct levels between 45% and 50% significantly increased the risk of cardiovascular death and major thrombosis compared with an Hct level managed to <45%>>
Current practice for women is less than 42-43 for best results.
I’ve only just read your reply. Presumably this applies to ET too? My haem always focusses on Hct - in addition to platelet count - and wants it <45. I didn’t think to question her but rather thought it must make sense.
It is the HCT that is the primary thrombosis risk factor with PV. There is not a linear relationship between PLT level and risk of thrombosis. It is also true that PLT absolute number does not have a linear relationship with thrombosis risk in ET. Higher PLT levels are associated with hemorrhage risk though. It is a bit complex, but the bottom line is that what may matter most regarding cytoreduction for PLT is the delta (degree of change) more than the absolute number on PLTs.
I would expect any MPN needs to watch HCT closely. My case is a good example with ET/PV overlap. I also had a brief HCT 50. something near my Dx. It went down on aspirin alone almost enough but at my age, and very high PLT, cytoreduction was called for.
As Hunter says, PLT is not clearly defined in absolute values. But to my knowledge the HCT numbers are an absolute goal for MPNs with clear data to back it up. So your Haem is consistent there.
At last count, it was 0.456. She wasn’t worried about the ‘6,’ but now I know she’s focussing on it, I will too. I’m still on 45mcg of PEG a week - if necessary, we can titrate up. My next CBC is on Mon, so I’ll know what’s happening by the following week and will post an update.
My HCT was fluttering up and below the 45% mark. My next Besremi dose will go from 110mcg to 150mcg. We will see how it goes. Not sure if your course of treatment is quite the same as mine. The bottom line is that since I have discontinued phlebotomy, my iron levels are increasing. This is driving up erythrocytosis. This is to be expected. Hopefully I will reach a balance of controlling HCT without phlebotomy and tolerable side effects from ROPEG. Hope you find the same with PEG.
The risk of thrombosis is more directly related to erythrocytosis than thrombocytosis.
The PLT levels do not directly correlate with risk of thrombosis. In fact, higher levels of PLT correlates with risk of hemorrhage. This has to do with come of the complexity of PLT function and von Willebrand factor activity. That is not to say PLT levels are not an issue, just that it is not the primary risk factor in PV.
The research has been very consistent in indicating the risk of thrombosis with PV is directly related to erythrocytosis with is roughly estimated using HCT. Note that this is actually a fuzzy measure as plasma volume also affects HCT. Thrombosis risk is lowered when the target HCT is maintained (45% for male, 42/43% for female). There reasons for this are complex. One of the factors is viscosity. Hyperviscosity causes a number of issues/risks (e.g. hypertension).
Part of the risk factors go beyond the numbers we look at with HCT and PLT. It is thought that the JAK2 mutation alters how blood cells behave. They become extra-sticky. This can cause them to stick to each other (thrombosis) and to stick to the vascular endothelium (microvascular symptoms).
When our blood is "too thick" (which is less than the max of the normal range) then we are a higher risk for thrombosis and microvascular symptoms. To reduce our risks we need to reduce viscosity (control HCT) and alter how the blood cells behave with blood thinning/anti-platelet medication (e.g. aspirin).
The alterations to how the blood cells behave is a key issue in managing PV risks. While it may be OK to ignore elevation in PLT above a target of 450, it would not be safe to ignore HCT above 45% for males or 42/43% for females.
I certainly understand wanting to avoid phlebotomies, or rather the chronic iron deficiency that is the intent of therapeutic phlebotomy. The adverse effects of chronic iron deficiency got worse the the PV symptoms for me. That is why I went on interferon treatment. I feel much better and it is doing a better job controlling all of my blood cell numbers.
Here is a plot I made of your HCT. Does it look right? Looks generally stable, with variations for both INFs. I added my guess of your doses/type. (no scales on the INF lines) I can adjust if this is not accurate.
Your WBCs and PLT seem uneventful thru all.
Your idea to go for 110mcg exactly matches mine, interesting, for same reasons. I will do it tomorrow. Agree the fat syringe makes such precision near hopeless.
My WBCs are somewhat higher so far, so in concept a bit more headroom to work with.
See next reply for comparison to my HCT (I posted before)
The chart looks right. I actually have responded really well to the interferons. Much better than to HU. The uptick in HCT is actually expected with increased Fe levels. Hopefully it will all balance out at the current dose.
Here is my latest HCT. My Dr says it's perfect at 44.1 Bes starts at Feb 1. Interesting that it's fairly stable, but there is a clear up trend since Bes without HU. I increased to 100mcg two weeks ago.
The HCT up trend corresponds approx to quitting the HU transition. But HU+ Bes did splat my WBCs counts. So this combo is likely no good for fixing HCT if WBCs are already low.
Makes sense to see the uptick in numbers with the d/c of HU. Increasing Besremi dose is certainly expected. Hopefully with the HU out of your system the potential drug interactions/potentiation will level out. Leukopenia is the noted HU-BES interaction.
I like seeing your interaction with your providers. As I learn more and more about my conditions, MM and MPN, I am also able to participate more in the decisions made. I can also better ask questions in order to understand the what’s and whys of treatment choices along with other aspects of my cancers. Thank you for your encouraging posts. I look forward to seeing more posts of your journey.
I started getting the rash while I was still on Pegasys. It would be a small pop-up rash that could be in most any location. About 4 inches in diameter. It was not related to injection location nor when the time of the injections. they did start to itch over time. Later, I also started to experience mild itching on broader areas of my body, usually on my back. This was deeper in the dermis and there was no evidence of rash on the surface of the skin. It was not severe, but certainly noticeable.
The pop-up rashes I treat with Eucrisa - a topical ointment. The broader areas of itching are clearly a histamine response. I am treating that with an antihistamine (Claritin). It works quite well to manage the itching.
Hi Hunter, Glad to hear your blood levels are presently under control. It never made much sense to me that dosing is to stepwise numbers based on the research rather than a continuum based on a patient- certainly the syringe I have for pegasys can be pretty precise. I mean I get it but why should one of the step numbers necessarily be appropriate for an individual. Your explanations of the PV blood nature helps as well - even if (with PV) I am in range for all the usual CBC parameters, my blood is not the same as others with the "stickyness" issue.
So from infrequent iron data, it seems that my iron recovers naturally in 4 to 6 months after a phlebotomy. For control of hematocrit, therefore, my needed dose of pegasys is variable based on my present level of iron. Like you, I would prefer to have my iron normal, so we are trying to establish the "normal-iron" pegasys dose (although so far my reaction to low iron has not been as bad as yours). But this isn't easy for the following reasons:
1. because of thrombotic risk, hematocrit should pretty much always be below 45 at all times.
2. interferon is slow to act - maybe months before dose is translated to reduction of erythrocytes.
3. iron is changing over time
4. white cells and platelets need to be within some kind of range.
5. side effects to all these things need to be reasonable.
6. other - like other conditions (in my case I had melanoma surgery and went off pegasys)
So far in my treatment, we have defaulted to a phlebotomy when needed to prevent the immediate risk of thrombosis (which is what you have to do). So I have had 4 phlebotomies in 1.5 years. Our goal is to somehow get past this cyclical pattern. My last blood hmct reading was 40.7 which is my lowest and may be producing some breathlessness and moving toward anemia. We recently increased pegasys dose to 135 mcg and the initial side effects seemed pretty bad, but maybe they would diminish after a couple of months. I am presently on 90 mcg. The doc is trying to get a little ahead of the iron recovery with the pegasys - but hard to do.
I guess the new iron drug (can't remember name, was PTG-300) might help in simplifying this - maybe in combination with interferon. It also seems that the interferon may produce changes over several years in the bone marrow that break this pattern.
So hunter- sorry if this is bit of a rant - but how my mind thinks of these things. Thanks for all your effort - I have learned a lot from all your posts. Appreciate all the kind people on the blog.
That is a really good job of explaining the intricacies of treating PV. It is all a balancing act, taking in a number of different factors. We need to reduce PV symptoms and risks while keeping the PV treatment side effects tolerable. All of our treatment options come with risks/benefits. We each experience different levels of efficacy and adverse effects. That is why individualized care my a MPN Specialist is so important.
It sounds like you are really on top of your treatment and have a sound plan in place. I would agree that it may very well make sense to add rusfertide (PTG-300) to your treatment plan when it becomes available. I would definitely add it to mine if tolerable doses of Besremi cannot control the erythrocytosis well enough to avoid phlebotomies.
My MPN Specialist wants me to stay between 40-45% on the HCT. At one point when i was over-phlebotomized HCT went all the way down to 32%. That was not a good place to be. I actually took iron pills for a short period of time. Yuck. Don't want to do that again.
I would note that there is a lot of range between 90 and 135mcg. If you are using a smaller syringe, dose titration is much easier at those lower doses. That is why I preferred using the smaller syringes and prepping by own injections from the PEG vial rather than a prefilled syringe. I hope that PharmaEssentia will move to something like that in the future. I do not think dose titration for PEG has to be done in 45mcg increments. Besremi dose titration does not need to be in 50mcg increments. We are each different. We each need to right dose for any one of us. This could well be something between the "standard" doses.
It remains interesting to me that my mpn doc had no qualms about increasing me from initial Besremi dose of 100mcg to 300 mcgs where I am now, in a matter of a few months. I noted that your dose increases are quite small compared to mine. Have you read or discussed any contraindications for over shooting Besremi dosage or is it just more of a cautious approach since the drug is fairly new? I questioned my doc on the quick dosage increase and he basically said that primary goal was to control hematocrit asap without phlebotomy and that 500 mcgs was the standard dose for Besremi in the most recent studies and there were no known major problems to speak of with that dose once it is determined the patient tolerates the initial doses. We are holding at 300 mcg for now pending labs but like you I would prefer the most conservatively low dose possible. Besremi is my first drug for hct controls and I realize that is relevant to higher initial dose and possibly rate of increase of dose. Like you I had a bad experience with low iron which for me was from many years of phlebotomies so that was my motivating factor for Besremi. Many of my low iron health problems have disappeared but now having very mild flu like symptoms randomly after the shot after getting to 300 mcgs when I had none with the lower doses. Still feel better than with lower iron so I want to power through and get the right dose to control hct. Sorry to keep harping on the dose issue but that seems to be the great unknown still with this drug at least for me. Thanks
Your concerns are perfectly reasonable. I have the same goal - keeping HCT <45% without phlebotomy. I have no desire to use any more Besremi (or previously Pegasys) to achieve this goal than is needed. Since I also experience thrombocytosis, controlling that is a good thing, but not a major focus of what we look at. The more comprehensive goal statement would be to achieve Complete Hematologic Response without phlebotomies. And without unacceptable adverse effects.
I had achieved a CHR with Pegasys prior to starting Besremi. So I started off at a good point for a lower dose. The issue is that as my iron levels continue to improve, erythropoiesis is increasing. This started while I was still on Pegasys. This is normal and expected. I may well need gradual increases in the Besremi dose to maintain CHR. However, I have been experiencing some side effects from the interferons. The most significant is leukopenia. The IFNs are decreasing production of all types of blood cells - RBC, PLT, and WBC. The latter is not such a good thing for me as my leukocytes were WNL. Now I am experiencing consistent lymphopenia and fluctuating neutropenia. I can afford to be a bit more neutropenic, but my LYMPH has dropped as low as 0.64. We do not want that to drop below 0.50.
I have also experienced some rashes and more generalized itching with the IFNs. It is well controlled with antihistamines and a topical ointment when needed; however, I would not want that to get any worse.
To be clear, we will increase my dose if needed to meet treatment goals. We will also monitor closely and see how i react if/when we need to do so. We each respond differently to Besremi (and the other meds) both in terms of efficacy and tolerance. We each need a different approach.
You are correct that there are different philosophies about how to approach this treatment. Some docs go with maximum level of the drug that the patient can tolerate to achieve maximum benefit. Other docs go with minimum level of the drug to achieve a treatment goal. The most important question is what is your philosophy? Treatment decisions (dose titration) needs to be based on your treatment goals, risk tolerance, and treatment preferences.
Thanks for weighing in on this discussion. All the best.
I think you are the reference point for max disclosed dosing on this forum. But so far it seems nothing really bad is happening at 300, great news.
My Dr explained that the WBC/HCT imbalance is to be expected with INF while HU, thru its different action, more often holds CHR balance.
Let's hope the HCT control on INF catches up over time. My question is whether pounding the INF harder is better than waiting for it to take full effect. (assuming counts are not too out of range)
Dosing interferon remains an experiment for all of us. Shame it can't all be standard.
On PTG-300 (Rusfertide) I asked my Dr about a low dose combo with INF to balance the HCT. He first said it's a long way from approval, but also said would not consider using it with INF. He didn't cite any contra indications, but I think he wants to see a trial 1st. I think it would be preferable to PLB if it were available.
I believe, there is a trial for rusfertide that allows entry if you have had a certain number of phlebotomies in last year and if you are on a stable dose of interferon for at least 6 months.
That would be helpful. If the approval includes that study I'd think my Dr would be ok with that. But maybe that requires going thru the PLB 1st, which would not really make sense in clinical use.
For now I don't think anyone here is yet stable with Bes anyway, as it is too new.
I may meet the criteria at some point with pegasys but its hard to be on a "stable" dose as it seems, at least for me, adjusted in response to my blood results. Maybe some day.
It does take some time for the IFN to work and get the dose adjusted. I had a bit of an advantage in that I was already on an IFN and at CHR when I switched to Besremi. We will all learn together how things will really pan out.
That is correct. It was either 2 or 3 phlebotomies in the last 6 months. Status of cytoreduction meds did not matter, Could be on HU or PEG and still get in.
So glad to see that things are going in the right direction for you. Your relationships with your care team is pretty impressive.
My platelets are still pretty high ( last count 845,000) but my situation is different since I don’t have PV, my red blood cell counts tend to be on the low side and I’m afraid some of these medications may make me anemic again. My doctor keeps wanting to increase my HU, but I’ve been resistant. I’m getting blood work done in a couple of weeks and if my platelets go over 1 million, I’ll probably just do that.
I have a wonderful care team. My two hematologists are great. They both listen to me and respect my right to make the decisions - always with their input. We work together as a team to manage my care. I have a few other "ologists" on the team. They likewise listen, answer questions, and respect my right to manage my own care. That is actually one of the key qualifications to be on my care team. Any provider that does not measure up is off the team.
Providers also have to work with the treatment goals that I set. This drives all treatment decisions. Right now we are working on one of my most important goals. I want to be "The World's Most Boring Patient." Alas, that goal remains a work in progress. My PCP seems to think that goal is hilarious. My Integrative Medicine doc said "The ship already sailed on that one." Note - I also like docs with a good sense of humor.
High platelets are relative. The current thinking is that the absolute number may not matter in terms of risk of thrombosis., though it does matter in terms of risk of hemorrhage. Dr mesa and other saddressed this at the recent MPN Conference. What matters more with platelet levels is the delta (the degree of change) than the absolute level. It will be interesting to learn more about this issue.
I canunderstand your reluctance to increase the HU. You are coirrect that will increase your risk of adverse effects, including anemia. I would wonder about some of your other treatment options, like Pegasys or Anagrelide or a combination therapy. Might be worth reviewing all of your options with a MPN Specialist.
Lovely to hear you have had some good news Hunter, you are always there and very helpful for everyone else. I hope it continues for you and wish you all the very best
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.