CONCLUSIONS: The combination of ibrutinib and rituximab provides superior PFS and OS relative to FCR for patients with previously untreated CLL age ≤70. These findings have immediate practice changing implications and establish ibrutinib-based therapy as the most efficacious first-line therapy for patients with CLL.
Written by
avzuclav
To view profiles and participate in discussions please or .
This study is what some have been waiting to hear, FCR head up against Ibrutinb. The graphs for both arms are good, but the ibrutinib results are no less than amazing. This abstract may mark the day the cll paradigm for treatment changed to non chemo for most all starting therapy.
Consider this language from the abstract, an abstract authored by some of the best:
"CONCLUSIONS: The combination of ibrutinib and rituximab provides superior PFS and OS relative to FCR for patients with previously untreated CLL age ≤70. These findings have immediate practice changing implications and establish ibrutinib-based therapy as the most efficacious first-line therapy for patients with CLL".
Immediate practice changing implications? That is huge. The survival curve for both is great, but for the IR arm is about perfect. I think it will look great at ten years too.
This is very strong data. But let’s not forget it’s actually possibly telling us that almost NONE of us who are treated first line are actually being treated with the right combination.
Notice that this study is looking so strong for a combo of ibrutinib PLUS rituximab not ibrutinib on its own. It seems likely tho this study doesn’t formally demonstrate it that the rituximab is contributing to the success seems here of the ibrutinib.
Also of course note that over all the results for both arms are good and many people did really well.
So we shouldn’t be too alarmed if we are currently or have recently been treated with a combination that turns out to not be best for patients as a whole.
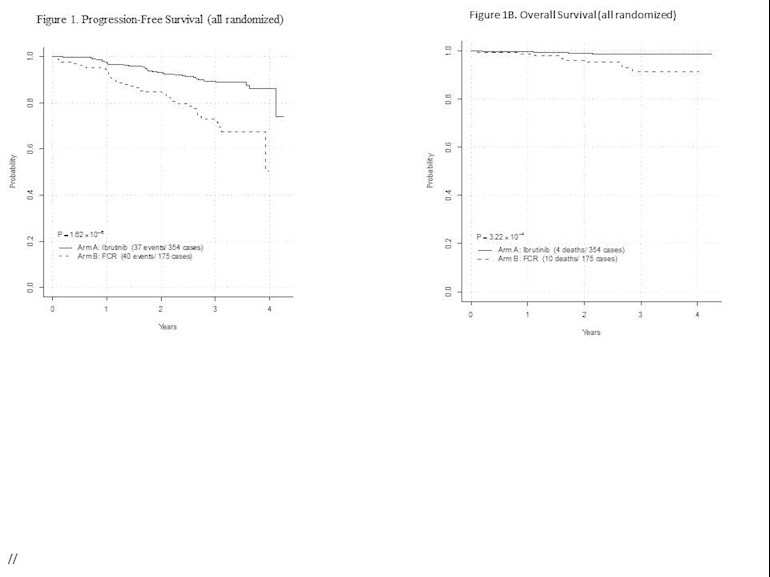
Note that overall in four years we are looking at just 10% of Ibrutinib taking patients having progressed requiring treatment and 23% of patients on FCR.
(Percentages calculated from the events and numbers listed on the graphs)
In terms of survival 1.1% of patients on I+R and 5.7% of patients on FCR had died by the end of four years of follow up.
We need to understand several things about the study which it sadly doesn’t answer in this report.
1. Did everyone who was intended to have six cycles of FCR actually get the six cycles or did some stop early (and were those some of the ones who relapsed and/or died?)
2. What did people who failed on FCR do after this study? Were they able to immediately Progress to ibrutinib on its own or with rituximab too outside of a study? Of those who relapsed and especially those who died what treatment were they able to have?
3. Are the FCR deaths all related to relapse or is there a toxicity issue and is there anything to learn about how FCR patients were treated here? Also is there anything we need to learn about the few patients who ended up progressing or dying on ibrutinb?
4. What proportion in each group reached MRD negativity and does that predict the outcome.
I have always tended to assume that once we started to get data that was head to head where FCR patients who relapsed were subsequently able to switch to ibrutinib we would no longer see an overall survival benefit for ibrutinib even if there was still a progression benefit. Ie if ibrutinib is such a good drug wouldn’t those who relapse do well if they are treated with it. I’m wondering if these patients typically only got ibrutinib mono therapy if they relapsed as that would be standard therapy at the moment (or did any of them get treated for a second time with FCR?)
Would there be a benefit in NOT waiting after FCR so long before switching to an novel combination (eg if someone only has partial response is that an indication we should immediately treat rather than wait for a relapse?)
Finally if there is an overall survival benefit to early treatment with an Ibrutinib containing treatment arm does this begin to call into question the whole “watch and wait for as long as you can” scenario?
Unfortunately I somehow doubt this will be quite as immediately practice changing as we might hope it would be.
And studies like FLAIR will still show us whether IplusR really is better than I alone or in fact V plus I or even V plus R or perhaps a combination of all three or their related medicines.
If this is the beginning of the end for FCR how are we going to make sure Ibrutinib containing therapies will be funded for everyone who needs them?
And if it really turns out that rituximab is vital to this picture how are we going to make sure Ibrutinib plus rituximab is available and not just ibrutinib?
It is worth remembering that the original FCR trial compared FC to FCR. As far as I remember they didn’t have an R monotherapy arm. Maybe the R really is the crucial bit (tho I don’t see enough here to warrant R on its own as opposed to part of a combination).
Finally given that venetoclax plus rituximab is already licensed second line is that going to turn out to also be an important option?
Is this a sign that what we need is novel combinations which include rituximab?
Just a few questions. Wish I was there when this was presented to ask some of them! Anyone know any more about this?
There were only seven late-breaking abstracts selected, two of which are CLL related. (The other is about the biology of a newly discovered venetoclax-resistant SNP in BCL2.)
These will be presented on ASH Tuesday (December 4th). If we're lucky, someone will post the slides from the oral presentation on the internet.
I’ll give you my amateur take. I think at the time this study was designed, it was not clear what the benefit would be of adding rutixumab to ibrutinib. Since that time I think other studies have shown ibrutinib does almost all the heavy lifting in that combination such that, if this trial was ibrutinib head up vs FCR, the results might be similar.
They can figure that out. I don’t think adding rituximab hurts or adds any significant degree of toxicity. The results of this large study are impressive and I do think signal that for doctors in countries where ibrutinib is available as a first choice, we will see it become the gold standard. Hopefully in countries where ibrutinib is less available, this study will accelerate its approval and use. I do understand the economics of getting approval for such an expensive drug and it’s impact on health care systems is complicated.
What the study does not address for me is sequencing. People who start on FCR will have a great option in their back pocket when and if they relapse, ibrutinib. Those who fail ibrutinib likely can’t do FCR. So we still need to see how the treatments compare 10 and 20 years out.
But hey Adrian, it’s pretty cool that we can both have a serious cancer and be discussing how it might impact us 10 and 20 years out, am I right?
And we haven’t even touched on where venetoclax fits in. Venetoclax might soon replace ibrutinib as the front line choice. More likely it will be some combination. It could be IVR that replaces FCR. Exciting times for sure.
One of my many questions to Dr Con Tam when looking at Ibrutinib + Venetoclax rather than FCR was whether this combo would rule out FCR if it failed. He said it shouldn't do so. I think I'd prefer another non-chemo treatment if needed but I wanted to ask to see how the novel agents limited future treatment options.
Closh, I might have been more clear in that I was writing in general. Generally speaking, most people who start therapy who have an FCR option are at or near 65, the cutoff age for most doctors to prescribe FCR. So for me, as a practical matter, FCR is not a viable back up option assuming ibrutinib takes me out 5 years or more.
Had I started with FCR, ibrutinib would be okay at any age. I am not regretting my ibrutinib choice, just observing that it probably precluded FCR for me. Bendustamine might still be an option as it is better tolerated for those over 65 than FCR.
But yes, for our younger members, FCR remains on the table so long as you are young and fit enough to take it.
Graham. thank's for weighing in with Dr Tam's thoughts on chemo after a non-chemo treatment as I too knew of no reason why "Those who fail ibrutinib likely can’t do FCR", particularly if Ibrutinib was their first treatment. If they had had chemo based treatment prior to Ibrutinib, then they may not benefit from another chemo based treatment, as they would be more likely to be 17p deleted.
In reality, no-one really knows, because most of the trial experience with non-chemo treatments has been on patients who have been previously treated with a chemo based treatment, then the common path after failing a non-chemo treatment is another non-chemo treatment. We haven't done the trials, primarily because of the expectation that chemo based treatments will soon be relegated to history. Can anyone recall a new chemo based treatment trial other than those based on Bendamustine, Fludarabine, Cyclophosphamide and Chlorambucil started in the last 10 years or so?
In summary, as Jeff says "it’s pretty cool that we can both have a serious cancer and be discussing how it might impact us 10 and 20 years out."
But those are the easier cases. I think the more impressive result is using two drugs (I+V) instead of four with more challenging patients and still getting 68% MRD-.
Also states: “With current follow-up, IR was also superior to FCR for IGHV unmutated patients (HR=0.262; 95% CI 0.137-0.498; p<0.0001) but not IGHV mutated patients (HR=0.435; 95% CI 0.140-0.1350; p=0.07).”
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")