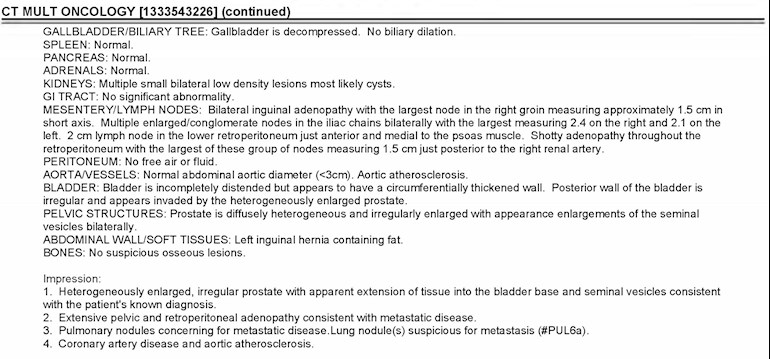
I have metastatic PC that has spread to the lymph nodes. The details of the spread are in the attached report. My primacy OC is at Kaiser. A doc at Stanford and another doc at Harvard, that I had asked for advice from, said that I should do hormone therapy for a few months, make sure that PSA is going down and if everything is reducing to start radiation of the area. My OC at Kaiser feels that adding radiation to Lupron + Zythiga does nothing for us and does not feel that I should do radiation. So confusing when doctors say different things.
What have people done in similar cases?
Written by
barrybayarea
To view profiles and participate in discussions please or .
You have extensive metastases in your lymph nodes and in your prostate. I don’t understand what value there is in treating your lymph nodes at this point. The HORRAD study showed that treating the prostate when there are extensive metastases does not contribute to survival. I think that docetaxel, Zytiga, Xtandi, and Erleada are all good choices ( but I think you should consider starting with docetaxel)
Are you saying that radiation does not make sense anymore? The doctors had suggested radiating both prostate and the lymph nodes - the whole pelvic area.
No, he is not confirmed M1, shotty adenopathy is not confirmed adenocarcinoma. He has suspicion of pulmonary area mets but not confirmed (Impression #3). There’s nothing in the above report that confirms distant LN’s are cancerous, needs to be confirmed.
I have to find out if I am M1, I suspect I am give the description but it is not mentioned in my rest reports. Another doc, not a prostate expert, just a friend, asked me if they had done a biopsy of my lymph nodes, which they have not. What if the lymph nodes are also something else like my lung nodes turned out to be. But I guess that is asking for too much
I had asked the doc today about starting docetaxel (chemo) since he did not want to do radiation, he had offered it as an option a month ago. He said since my lung liasons turned out to be carcinoid tumor and not prostate cancer, as earier diagnosed, I do not qualify for chemo until the cancer becomes castration resistant.
Docetaxel is approved for newly diagnosed metastatic hormone sensitive PC (mHSPC). You do not have to wait for castration resistance, not even at Kaiser. All the drugs I mentioned (including docetaxel) are already FDA approved for mHSPC:
I know it is approved, the doc had offered it to me before when he thought I had PC in the lungs too, now he said the US study that was done, does not quote any advantage from chemo vs double hormone therapy (Lupron + Zytiga). He said since you are already on that path of hormone therapy stick with until it stops working and then we will do the chemo.
The reason I prefer chemo first is this: if you start with chemo, you can move onto Zytiga in 15 weeks; if you start with Zytiga, it may take 3 years until you get to try chemo.
I would have preferred it too. They did not start it initially as they wanted to see if my lung modules reduce with ADT, confirming that it is PC. At the time they had not done the biopsy as it was considered dangerous, the 1cm target being 8cm deep. They thought if the lung thing was a different cancer, chemo might hide it and they will never know if it needs to be treated differently. When it did not respond to ADT they ad to do the biopsy to confirm.
Just a question to a person has alot of information, Dr is thinking of starting me on generic zygtiga if the psa continues to go up but I would rather start with arbitrone , it is zero copay on Medicare. He is pushing the more expensive drugs but rather start with cheaper until it fails. My psa was 4.1, then 3.9 now 3.6, he is waiting for it to level off. Have my lupron shot next month on the 13 the and see him for follow up on March 12th. How long does the generic of casadex last before having to the next drugs and how long does zygtiga last in most cases. Thank you for your answers, live on. The most recent scans, bone and CT shows no disease progression and no new Mets. He did mention the microscopic cells that could blossom out.
Sorry, he wanted to use the abritone but I would rather start with the generic of casadex until it fails. The generic casadex is zero pay , the genetic of zgytia is 1300. I am thinking of the first line of defense of genetic casadex then move to the next drug. He says that the casadex is not as strong as the more expensive stuff. I guess some thoughts on the drug progression to keep psa in check and on the low end.
Hi Allen. My name is Dennis Savini I’m a member here but have been writing my book so I don’t spend a lot of time online. Was diagnosed almost 5 years ago with stage four metastatic prostate cancer to the bones and a lymph node. Started with casodex, on to Lupron , Xygeva injections once a month, and 4 pill of Zytiga and 10 mg of prednisone. PSA after a heat dropped to 0 last month it went up to 1 my oncologist Dr. Nahum said there was nothing to worry about, I also get these small bumps on my chest that do not react to sun. Any input at all would be appreciated, I eat healthy, try to exercise, but am very weak, I’ll be 71 next month, also the only relief I get is from Vicodin and still have a broken tooth and AH. Brother is a dentist! Ok any input at your convenience is greatly appreciated. Also vertigo comes ang Goes! Thanks so much for this soothing site and group of fellow warriors! Dennis. Aka captsquid
(2) try switching to dexamethasone from prednisone.
Also, ask your doctor to prescribe Celebrex. It may increase survival in combination with Xgeva (it does with Zometa). Also, it may allow you to cut back on Vicodin.
Thanks so much Tall_Allen! I’m not stopping the Zytiga, do you think I should? Thanks so much for quick response! Love this group just need to finish my novel , which has the main character later in life goes through what I’ve gone through. Thanks Again!
Most on this forum would advise to treat the prostate as well as radiation to the pelvic bed. I was stage t3bN1M0 +SV (mesorectal node) and did successful HDR-Brachy + IMRT (see profile). Schedule a consult with Dr Chang at UCLA.
I can consult with Dr Chang but I do not have a PPO plan, I have to get my treatment done at Kaiser. Somehow I have to convince my Kaiser doc to do it without having to pay for it from my pocket.
IMO, it’s worth your time to discuss with a Brachy RO in Kaiser or outside to get another opinion. If you are still M0, and that means only LN mets below the common iliac artery bifurcation, I would definitely radiate the prostate and pelvis no matter how many LN+. Dr Chang came from USF, and has a replacement there, see if you can find out and get a consult. I didn’t see any indication that you have bone mets, but you need to get a PSMA scan before you start ADT to find out.
Is Branchy RO - radiation oncologist? Not sure what M0 is, it is first stage mets i.e. in lymph nodes (LN)? That is what I have, just LN, bone scan is clear. My OC said that my mets were too high to be radiated, below my kidneys and parallel to my liver. I started Lupron in Oct and added Zytiga 4-weeks ago, so far PSA has been declining stedily. Last 4 months - before ADT 32, 43, after ADT 2.2, 0.7.
M0 = non-metastatic, where metastatic = met to bone or met to a distant LN (above the iliac artery bifur)
So if the mets near your kidneys are considered distant mets, it would be M1. Please clarify if you are M0 or M1.
If M0, the you can be treated locally with HDR-BT and followed up with a 25 session IMRT (per my profile).
Even if you are M1, but have <5 bone mets, i.e., oligometastatic, Brachy tx plan still applies, but it is a gray area if there are multiple distant LN mets near organs, which is what your Dr has opined that it is not treatable with radiation.
Mine is similar as we all are. I only had the one opinion. Mine. I feel the Dr didn't give me all the info and really hate that.
I had my prostate completely removed and was told that would be in place of chemo and radiation.
2 weeks after surgery Dr tells me the surgery went well but the next step was chemo and radiation. I was pissed. Anyway he says while removing prostate he had to remove surrounding lymph nodes and scrap seminal vesicles and surrounding area.
Radiation is to make sure nothing was left and kill what remains. I had all tests done prior and it was isolated to only prostate...supposedly. Not on the bones or anywhere else at that point. Your report looks like it has metastasized to other parts... is it in the lungs?
Your Dr may not want to do much because of the reaction. Tell me more about the spread.
No it is not in the lungs. Initially they said it might be but then a biopsy showed that the lung thing is not PCA and may not be anything, can be ignored for now.
I agree with Tall Allen. Because you have multiple soft tissue mets, then external beam radiation is impossible to do to all of them, so systemic treatment must be used, such as chemo. This may not work, and if it does not, then I'd suggest getting PsMa Ga68 PET/CT scans and possible FDG scans to better view what your Pca status is. Then you could get Lu177 and possibly get Olaparib PARP inhibitors and that's about the best you might do now.
You have a very serious case of Pca.
But your docs are not saying Pca is in bones. Lu177 can work of all soft tissue mets that you have. ditto PARP inhibitors.
Radiating the whole pelvic area with enough radiation to kill all Pca present is extremely risky and you sure will not like the side effects. I had 70 Grey EBRT to the PG in 2010 and it hardly killed any Pca, and I had bad side effects. Having 70 Grey to ALL things in your pelvic area would be distressing for a long long time, IMHO.
The only reason I am alive after diagnosis in 2009 was that I had regular Psa checks because I expected to get it, because there was so much cancer in my family tree. When Psa hit 5.0, I arranged for biopsy, but then docs found I was inoperable but mets were not found, maybe because they were too small to see in scans. I had ADT for years than added Cosadex, then Zytiga, then as these failed one after I got chemo when Psa was 12. Chemo failed after 5 shots so I had 4 shots of Lu177 last year and Psa is now 0.3, so seems like I am doing OK and docs have not told me yet that I need to have PARP treatment for mutated Pca that Lu177 won't fix. I am also taking Xtandi now. So I have lasted over 10 years at 72yo since diagnosis which was too late in 2009. It should have been when Psa was 3.0 in about 2004 when I bet Gleason score was 5, not 9 like in 2009, and then RP may have fixed me before I had any mets.
But we don't get to travel back in time and do what we should have done earlier.
Bills was in lymphs. ( found on surg). He has been seeing Dr. Kwon at Mayo for close to 5 years. Had chemo, then 18 mo of zytiga,Lupron, prednisone, 6 mo into that, 37 radiation. Has been non detectable and no evidence of disease on c11 choline pet scans for over 3 years, on no meds or treatments over 2 years. Has PSA every 3 mo yearly scan and MRI.
I ran into the same issue back when I was dx in 2014. I had extensive mets throughout my skeleton and in several nodes - G9 PCa. My RO recommended radiating (debulking) the prostate and as many of the affected nodes as he could safely. He said it could help get more time out of HT and prevent prostate mets from spreading to nearby tissue where it is very difficult to treat.
My uro was against it said it was too risky, my MO said it was a good idea and after reading Snuffy Myers book it seemed to support debulking the primary tumor and as much cancer as possible. So after a lot of thought, research and discussion I decided to go ahead with it. I was on ADT for 6 months prior to IMRT. My RO said it would make treatment easier and more effective and that there was a synergy between the two.
Going on 6 years now since dx and PSA still undetectable. Now I’ve also had chemo per CHAARTED, continue on ADT, etc. I’ve taken an aggressive approach and radiation was a part of it. When I was a patient of Snuffy Myers he once commented that radiating my prostate was one of the best things I could have done “eliminating the mother ship”. For me I feel it was a critical part of my treatment.
See my profile. I had radiation to all pelvic lymph nodes in 2015 after SRT in 2014 to prostate bed and RP in 2013. But my recurrence was sequential. No recurrence in any areas radiated and I never used second line ADT lik Zytiga Unless you consider estradiol patches second line.
Hello. So you are saying the radiation did kill anything that was in the initial affected areas?
I start radiation in 14 days and this is a backup to the complete removal of my prostate about 4 months ago. I'm 51 and really trying to understand what I should do?
Yes apparently it did. Every area I radiated and I did it to prostate bed, all pelvic lymph nodes, right femur , left third rib and right scapula have shown no recurrence.
I would support the perspective of Tall Allen. Get a biopsy of a lesion wherever you can to confirm and get genetic info. It could be unwise to treat based upon the hope of best-case presumptions and must consider that lesions strongly suspicious for metastasis are likely just that. Doing docetaxel early (now) has survival advantage and earlier will be easier to tolerate than later. Then you can start ADT fairly soon and opt for the radiation within just a few months, as EdBar experienced. The radiation can give an abscopal effect of triggering a strong immune response to the non-irradiated mets wherever they may be.
Ga-PSMA scan also a good idea and opens consideration for Lu-PSMA treatment later.
Be strong and steady in your decisions at this time. We know it is very difficult to navigate when your life is on the line.
If it were me, I would opt for the chemo because of your Gleason. Try stopping things systemically as early as possible. PSMA scan would be a good idea.
Thank you everyone for your very valuebale feedback, it is very helpful. My plan for now -
1. See a radiation oncologist and see what he thinks about radiating the pelvic region.
2. Try to insist on a PSMA scan and a biopsy of the lymph nodes - the doc has been resisitant in the past.
3. Once the dust settles and all reports are in, go back to inisiting on chemo soon and not wait for the cancer to become castration resisitant.
I did see in the article that tall_allen posted that adding radiation may only add 2-months to your life, according to that study the median went from 45-months to 47-months only. Will keep that in consideration.
Some more background -
No bone mets, only lymph nodes for now.
Did gene testing, result was negative both for my clean sample and the tumor itself. No inherited genes and no alternation detected.
One thing worried me about my visit with my OC yesterday, he said if you were in UCSF (where he used to work) they might give up radiation with lymph nodes effected that high up but not at Kaiser. I did not say anything but in my mind I was thinking maybe I should be at UCSF. Going to try to see if I can buy a PPO insurance. I do not qualify for medicare yet, I am 55.
Excellent posts troops, very proud of the input given this fellow!!!!!
How old are you? I think we should be looking at age as well as general health in terms of treatment options, when at this stage.
My major concern is your high gleason score coupled with the fact that you all pc in all cores, i.e. it had to have spread by this point in time.
I do think you have to get going on something to start the battle.
There are just so many variables involved, for anyone to make a call as to what to do, and this also is in large part why you get different advice from your med crew.
I like blasting if you can get rid of a pile of pc in the process.
Your buying time now so do not panic as to their only being one path to follow for as noted here, you have several and some overlap. I think you also have to look at quality of life in the mix, as the more aggressive treatments definitely have larger negative impact on the body as a whole.
Good luck, stay tuned for your new family is here and the boys will be at your side every step of the way!!!
Just to followup, spoke to my doc. He has given me a consult with a radiation Oncologist. He also suggested we redo the CT and bone scans (last ones were in Oct) to see the current situation, now scheduled for 28th Jan. While my bone scan was negative the last time, he said sometimes after hormone theraphy there is a "flare up" effect and cells not visible before show up. He would not do a PSMA scan, said it not "approved". Guess people do this outside of their hospitals? I will have to find a location near me in the Bay Area.
Like billyboy3 said, you guys are awesome, such a wealth of information. I had emailed my doc yesterday, saying, I am not trying to be a difficult patient, just trying to do what I can to survive. Being a single parent to a 10-year old (he lost his mother to brain cancer Feb 2019) is not easy. I will give this fight all that I can, that way I will not repent later. For my son's sake, I have to find a way to be around at least until he turns 18 and sometimes that may mean grasping at straws.
A heartfelt thank you to everyone for your excellent advise and guidance, much appreciated!
Seems like my case may a bit different from your husband. My cancer has spread all through my lymph nodes and I cannot have surgery anymore. Reading your other post, I think, like other people suggested, you need to first see if the cancer has spread and how extensive the spread is and to what parts. My doctor at Kaiser thought that radaition will not help but then I switched to UCSF. The doc there thinks radiation will help. If the Covid-19 restrictions lift OK, I should be starting radiation in end of June to the prostate and all the effected lymph nodes, that they can see. I am currently on Lupron, Zytiga and Prednisone. My PSA reading has been steady at around 0.2 the last few months.
Please let me know if I can answer any more questions. Best of luck to the both of you.
Well my husband got the psma pet scan at UCLA, paid cash. It showed no bone or organ mets! Does have some pelvic region lymph nodes which is why his post rp psa is 4. He started lupron and zytiga and prednisone. Probably radiation next.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")