From paper
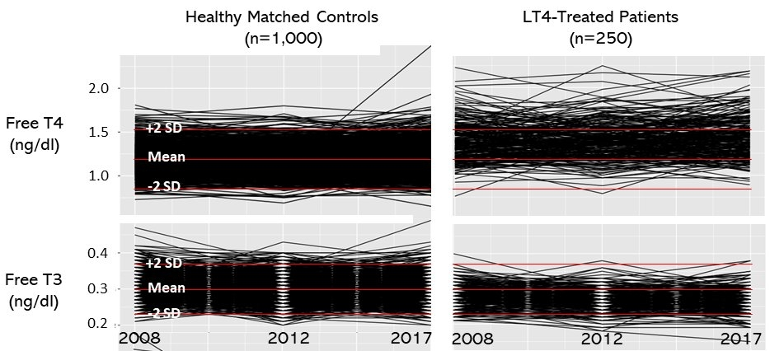
Antonio C Bianco has posted on Twitter about this new paper (of which he is a listed author). The first quote below has the image above attached. The second quote has a different image from the paper.
Can this be called normal? Look at T4 and T3 levels in LT4-treated patients with normal TSH. T4 stays high and T3 drops to the bottom of the reference range. This goes on for years, for the duration of the treatment.
twitter.com/Bianco_Lab/stat...
Another view of the same problem. In LT4-treated patients, FT4 distribution shifts to the right and FT3 to the left. While TSH remains normal, many patients have above-normal FT4 and sub-normal FT3 levels. Can we call this "normalization of thyroid function tests"?
twitter.com/Bianco_Lab/stat...
Thyroid hormone homeostasis in levothyroxine-treated patients: Findings from ELSA-Brasil
Gustavo C Penna 1 2 , Isabela M Bensenor 3 , Antonio C Bianco 1 , Matthew D Ettleson 1
Affiliations
PMID: 38506164
DOI: 10.1210/clinem/dgae139
Abstract
Context: The effectiveness of levothyroxine (LT4) in restoring thyroid hormone (TH) homeostasis, particularly serum thyroxine (T4) and triiodothyronine (T3) levels, remains debatable.
Objective: To assess TH homeostasis in LT4-treated individuals using data from the Longitudinal Study of Adult Health in Brazil (ELSA-Brasil) study.
Methods:
The ELSA-Brasil study follows 15,105 adult Brazilians (aged 35 to 74 years) over 8.2 years (2008-2019) with 3 observation points assessing health parameters including serum thyroid stimulating hormone (TSH), free T4 (FT4), and free T3 (FT3) levels. We analyzed 186 participants that initiated treatment with LT4 during the study, and 243 individuals continuously treated with LT4 therapy.
Results:
Initiation of therapy with LT4 resulted in a 11-19% decrease in TSH, a ∼19% increase in FT4, and a 7% reduction in FT3 serum levels (FT3 dropped >10% in ∼40% of the LT4-treated patients). This was associated with an increase in triglyceride levels and utilization of hypolipidemic and anti-diabetic medications. Participants continuously treated with LT4 exhibited a stable elevation in serum FT4 and, a reduction in serum FT3 and TSH levels. While 115 participants (47.3%) had at least one serum FT4 levels above the control reference range (>1.52 ng/dL), 38 participants (15.6%) had at least one serum FT3 below the reference range (<0.23 ng/dL).
Conclusion:
The present results challenge the dogma that treatment with LT4 for hypothyroidism restores TH homeostasis in all patients. A substantial number of LT4-treated patients exhibit repeated FT4 and FT3 levels outside the normal reference range, despite normal TSH levels. Further studies are needed to define the clinical implications of these findings.
Keywords: TSH; hypothyroidism; levothyroxine; thyroxine; triiodothyronine.
Abstract accessible here:
pubmed.ncbi.nlm.nih.gov/385...
(Apologies, I originally thought the full paper was accessible. Correction made.)

")